Up next in 10

What is Plasmodium vivax? The Malaria Parasite Explained
Website: https://biologynotesonline.com/
Facebook: https://www.facebook.com/biologynotesonline
Instagram: https://www.instagram.com/biologynotesonline/?hl=en
Show More Show Less View Video Transcript
0:00
Hey everyone. Today we're diving into
0:02
the fascinating world of a tiny but
0:04
mighty parasite that affects millions of
0:06
people worldwide. We're exploring
0:08
plasmodium vivac, a microscopic parasite
0:11
that causes one of the most important
0:13
infectious diseases in human history,
0:15
malaria.
0:17
Here's what plasmodium vivax looks like
0:19
under a microscope. You can see it
0:22
highlighted among the red blood cells
0:24
where it lives and multiplies during
0:26
infection. Here's a crucial fact to
0:28
remember. Plasmodium vivax is the most
0:31
common cause of recurring malaria
0:33
worldwide. This means it can come back
0:35
again and again even after treatment.
0:38
While pivox is generally less deadly
0:41
than its cousin plasmodium falsiparum,
0:43
it's still a serious health threat.
0:45
Palsiparum causes more severe
0:48
complications and can be a medical
0:49
emergency. But pivox has its own
0:52
challenges with recurring infections.
0:55
Understanding plasmodium vivax is
0:57
crucial for global health efforts and
0:59
malaria elimination programs worldwide.
1:02
So let's dive in and explore this
1:04
fascinating parasite together. Learning
1:06
about its life cycle, how it affects
1:08
humans, and what we can do to fight it.
1:12
Plasmodium vivax is a protoonean
1:14
parasite. But what exactly does that
1:16
mean? Let's break this down step by
1:18
step. First, let's understand what a
1:20
protozonean is. A protozonean is a
1:23
single-sellled organism. Imagine the
1:25
tiniest living thing you can think of
1:27
made up of just one cell but still
1:29
capable of complex behaviors. Plasmodium
1:32
vivax belongs to a specific group of
1:34
protoones called amplexa. This group
1:37
includes many parasites that are spore
1:39
forming and need hosts to survive. Now
1:41
here's what makes plasmodium vivac
1:44
special. It's a parasite that needs two
1:46
different hosts to complete its life
1:48
cycle. It uses both humans and
1:50
mosquitoes, moving between them to
1:52
survive and reproduce. What makes
1:55
plasmodium vivax particularly
1:57
troublesome is that it causes recurring
1:59
malaria. Unlike some other types of
2:01
malaria, vivac malaria can come back
2:04
weeks or even months after you think
2:06
you've been cured. Here's what
2:08
plasmodium vivax actually looks like
2:10
when it infects human blood cells. These
2:12
dark purple clusters you see inside the
2:14
red blood cells are the parasites
2:17
actively feeding and multiplying.
2:19
So to summarize, plasmodium vivax is a
2:22
single-sellled parasite that needs both
2:25
humans and mosquitoes to survive and
2:27
it's the main cause of recurring malaria
2:29
making it a persistent global health
2:31
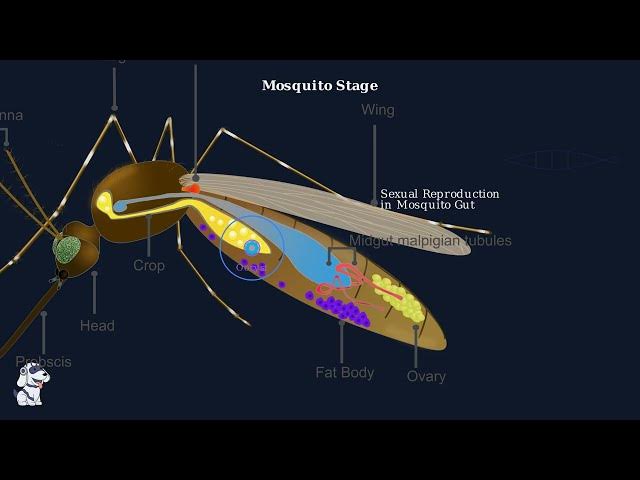
challenge. Mosquito stage of the
2:33
plasmodium vivac life cycle is where the
2:36
parasite underos sexual reproduction.
2:38
This critical phase transforms the
2:40
parasite from its human blood form into
2:43
an infectious form ready to infect the
2:45
next human host. When a female anophles
2:48
mosquito takes a blood meal from an
2:50
infected person, she doesn't just ingest
2:52
blood cells. She also sucks up special
2:55
sexual forms of the parasite called
2:57
gtoytes. Inside the mosquito's gut,
3:00
these gittotes undergo sexual
3:02
reproduction. Male and female gimitoytes
3:04
fuse together to form zygot beginning
3:06
the sporagonic cycle. The zygote
3:09
develops into a motile ucinite which
3:12
penetrates the mosquito's gut wall and
3:14
forms an oyst. Inside this oyst
3:17
thousands of sporzoids develop through
3:19
multiple rounds of division. When the
3:21
oicyst matures and bursts, thousands of
3:24
sporzoids are released. These sporzoids
3:27
then migrate through the mosquito's body
3:28
cavity to reach the salivary glands.
3:31
Once the sporzoids reach the salivary
3:34
glands, the mosquito becomes infective.
3:36
The entire sporagogonic cycle takes
3:39
about 10 to 14 days depending on
3:42
temperature. The mosquito is now ready
3:44
to transmit plasmodium vivax to the next
3:46
human host through her next blood meal.
3:49
When an infected mosquito bites a human,
3:51
it injects thousands of microscopic
3:54
parasites called sporzoids directly into
3:56
the bloodstream. This marks the
3:58
beginning of the human stage of the
4:00
plasmodium vivac life cycle. These
4:03
sporzoids are highly motile and move
4:05
rapidly through the bloodstream. They
4:07
have a specific target, the liver.
4:10
Within minutes of injection, they begin
4:12
their journey to find and invade liver
4:14
cells. The sporzoids specifically target
4:16
liver cells, also called hpatocytes.
4:19
Once they reach the liver, they actively
4:21
invade these cells by penetrating the
4:24
cell membrane. This invasion process is
4:26
remarkably efficient. Once inside the
4:29
liver cells, the sporzoids transform and
4:31
begin multiplying asexually. This
4:34
process is called schizogy. A single
4:37
sporzoid can produce thousands of new
4:39
parasites called mezzoids. This
4:41
multiplication happens completely hidden
4:43
from the immune system. This liver stage
4:46
typically lasts 8 to 15 days in
4:48
plasmodium vivax infections. During this
4:51
time, the infected person shows no
4:53
symptoms. They appear completely
4:55
healthy. However, thousands of parasites
4:58
are multiplying inside their liver cells
5:00
preparing for the next phase of
5:02
infection.
5:04
Now we come to one of the most
5:06
fascinating and dangerous aspects of
5:08
plasmodium vivax, the formation of
5:10
hypnosits.
5:12
These are the hidden threat that makes
5:14
vivac malaria so challenging to
5:16
eliminate. After the sporzoids enter the
5:18
liver, something remarkable happens. Not
5:21
all of them immediately develop into
5:23
schizants. Some transform into a
5:25
completely different form called
5:27
hypnosits. When sporosoids reach the
5:29
liver, they face a critical decision
5:31
point. Some will continue the normal
5:34
development cycle, but others will enter
5:36
a state of dormcancy.
5:38
The word hypnosate literally means
5:41
sleeping animal. These dormant forms are
5:43
much smaller than the actively
5:45
developing parasites and remain
5:47
completely inactive in liver cells.
5:51
The remarkable thing about hypnosits is
5:53
how long they can remain dormant. They
5:56
can stay inactive for weeks, months, or
5:58
even years without causing any symptoms
6:01
whatsoever. During this entire dormcancy
6:03
period, the person feels completely
6:05
healthy. There are no symptoms, no
6:07
fever, no indication that these time
6:10
bombs are quietly waiting in their liver
6:12
cells.
6:14
Scientists can detect hypnosit
6:16
infections by measuring antibbody
6:17
responses over time. This research image
6:20
shows how antibbody levels change and
6:23
helps classify different types of vivax
6:25
infections based on these immune
6:27
responses.
6:29
Think of hypnosits as biological time
6:31
bombs. They sit quietly in liver cells
6:34
completely undetected until something
6:36
triggers their reactivation.
6:38
This could be stress, illness,
6:40
pregnancy, or sometimes for no apparent
6:42
reason at all. When hypnosits finally
6:44
reactivate, they explode into action,
6:47
rapidly multiplying and releasing
6:49
thousands of new parasites into the
6:51
bloodstream. This causes a relapse, a
6:54
new episode of malaria that can be just
6:56
as severe as the original infection.
6:59
This is why hypnosits are considered the
7:01
hidden threat of vivax malaria. They
7:05
make the disease incredibly difficult to
7:06
eliminate because even after successful
7:09
treatment of the blood stage, these
7:11
dormant forms can reactivate months or
7:13
years later, causing new infections and
7:16
continuing the cycle of transmission.
7:20
Now we reach a critical phase in the
7:22
plasmodium vivac life cycle. After
7:25
developing in the liver for about a
7:27
week, the parasites are ready to enter
7:30
the bloodstream and cause the symptoms
7:32
we associate with malaria. The mature
7:34
liver skits rupture, releasing thousands
7:36
of mezzoids into the bloodstream. These
7:39
mezzoids are now programmed to seek out
7:41
and invade red blood cells. Here's where
7:44
plasmodium vivax shows its preference.
7:47
Unlike other malaria parasites, Pivax
7:49
specifically targets reticulosytes,
7:52
young immature red blood cells that are
7:54
easier to invade. The morazzo attach to
7:57
and invade the reticulosytes. Once
7:59
inside, they transform and begin to
8:01
multiply through a process called
8:03
schizogy. Inside the red blood cell,
8:06
each mezzoid develops into a trophosoid,
8:08
then a skidzant. The skids divides
8:11
multiple times, creating 12 to 24 new
8:14
mezzoids within a single cell. After 48
8:17
hours, the infected red blood cell
8:19
bursts open, releasing 12 to 24 new
8:22
mezzoids into the bloodstream. This
8:24
synchronized bursting of millions of
8:26
infected cells is what causes the
8:28
characteristic fever spikes of malaria.
8:31
This creates a vicious cycle. The newly
8:34
released mezzoids seek out fresh red
8:36
blood cells to invade and the process
8:38
repeats every 48 hours. Each cycle
8:41
releases toxins and cellular debris that
8:44
trigger the body's immune response
8:46
causing fever, chills, and other malaria
8:48
symptoms. This bloodstream infection
8:50
phase is what makes malaria so
8:53
dangerous. The synchronized destruction
8:55
of red blood cells every 48 hours
8:58
creates the classic pattern of recurring
9:00
fever and chills that patients
9:02
experience while also reducing the
9:04
blood's ability to carry oxygen
9:06
throughout the body. Vivax malaria
9:09
presents with a characteristic set of
9:11
symptoms that patients and health care
9:13
providers should recognize.
9:15
Understanding these symptoms is crucial
9:17
for early diagnosis and treatment.
9:20
The most common symptoms include
9:22
recurring fever with chills and
9:24
sweating, severe headaches, muscle aches
9:26
throughout the body, and nausea. These
9:29
symptoms often occur in cycles,
9:31
typically every 48 hours, corresponding
9:33
to the parasites reproduction cycle in
9:36
red blood cells. However, vivax malaria
9:39
can also lead to more serious
9:41
complications. Let's examine the
9:43
symptoms of severe anemia which is one
9:45
of the most dangerous complications of
9:47
this disease. Severe anemia is a serious
9:50
complication of vivax malaria. As shown
9:53
in this diagram, anemia causes fatigue,
9:56
weakness, shortness of breath,
9:57
dizziness, headaches, and pale skin. The
10:00
comparison shows normal blood with
10:02
healthy red blood cells versus anemic
10:04
blood with fewer red blood cells. To
10:06
understand why Vivvac malaria causes
10:08
these specific patterns, we need to
10:11
examine how this parasite targets young
10:13
red blood cells called reticulosytes.
10:16
This diagram shows red blood cell
10:18
development from stem cells to mature
10:20
red blood cells. Plasmodium vivacly
10:23
targets reticulosytes which are young
10:26
red blood cells that still contain some
10:28
cellular machinery.
10:30
This preference means parasite levels in
10:32
the blood are generally lower than with
10:34
falsiperm malaria. But the infection can
10:36
still cause severe complications.
10:39
Despite lower parasite levels, vivax
10:42
malaria can still cause life-threatening
10:44
complications, especially in vulnerable
10:46
populations. Severe complications of
10:49
vivac malaria include respiratory
10:51
distress and severe anemia. Infants are
10:54
at particularly high risk for these
10:56
life-threatening complications. Their
10:59
developing immune systems and smaller
11:01
blood volumes make them more susceptible
11:03
to the effects of red blood cell
11:04
destruction caused by the parasite.
11:07
The key takeaway is that while Vivvac
11:10
malaria symptoms may seem milder due to
11:12
lower parasite levels, this infection
11:15
should never be underestimated. Early
11:17
recognition of symptoms and prompt
11:19
medical attention are essential,
11:21
especially for infants and young
11:23
children who face the greatest risk of
11:24
severe complications.
11:27
Pivax malaria has a widespread global
11:30
distribution affecting millions of
11:32
people across multiple continents.
11:35
Understanding where this parasite is
11:36
most common helps us target our
11:39
prevention and treatment efforts
11:40
effectively. Pivax is found primarily in
11:43
five major regions around the world.
11:46
These include the Middle East, Asia, the
11:48
Western Pacific Islands, Central
11:50
America, and South America. The global
11:52
impact is significant. In 2020 alone,
11:56
Pivax caused an estimated 4.5 million
11:58
malaria cases worldwide. More than
12:01
onethird of the world's population lives
12:03
in areas where they could potentially be
12:05
infected with this parasite. Pivax is
12:08
particularly common in two regions, the
12:10
Americas and Southeast Asia. These red
12:13
dots show areas of highest prevalence
12:15
where the parasite causes the most cases
12:18
and poses the greatest public health
12:19
challenge. Other regions like parts of
12:22
Asia and the Middle East have medium
12:24
levels of P vivvax transmission shown by
12:27
these orange dots. The intensity varies
12:29
based on factors like climate, mosquito
12:32
populations, and local control measures.
12:35
This geographic distribution pattern is
12:37
crucial for global health planning.
12:39
Countries in high prevalence regions
12:41
need robust malaria control programs
12:44
while those in medium prevalence areas
12:46
can focus on targeted interventions and
12:48
surveillance to prevent outbreaks.
12:51
Understanding pivac distribution also
12:53
helps researchers and policymakers
12:55
allocate resources effectively develop
12:58
region specific treatment guidelines and
13:00
coordinate international efforts to
13:03
reduce the global burden of this
13:05
persistent form of malaria. Accurate
13:07
diagnosis is crucial for effective
13:09
malaria treatment. There are two main
13:11
methods used to detect plasmodium vivax
13:13
in patients. Microscopic examination and
13:16
molecular testing. The most common and
13:19
traditional method is microscopic
13:21
examination. A trained laboratory
13:24
technician takes a blood sample from the
13:26
patient and examines it under a
13:27
microscope to identify malaria parasites
13:30
inside the red blood cells. Here's what
13:32
a technician actually sees under the
13:35
microscope. This image shows red blood
13:37
cells with malaria parasites visible as
13:40
dark spots inside some of the cells. The
13:43
parasites appear as ring-shaped or more
13:45
complex forms depending on their stage
13:47
of development. While microscopic
13:50
examination is reliable, it has
13:52
limitations. When parasite levels are
13:54
very low, they can be difficult to
13:56
detect. This is where molecular testing
13:59
becomes valuable. Molecular tests like
14:01
PCR detect the genetic material of the
14:03
parasite rather than looking for the
14:05
parasite itself. These tests are much
14:08
more sensitive and can detect very low
14:10
levels of parasites that might be missed
14:12
by microscopy. Both methods have their
14:15
place in malaria diagnosis. Microscopy
14:17
is faster and less expensive, making it
14:20
ideal for areas with limited resources.
14:22
PCR is more accurate for detecting
14:24
low-level infections, but requires
14:26
specialized equipment and trained
14:28
personnel. The key takeaway is that
14:31
accurate diagnosis is the first step in
14:33
treating malaria effectively. Health
14:35
care providers choose the diagnostic
14:37
method based on available resources,
14:40
urgency of results, and suspected
14:42
parasite levels in the patient. When
14:45
someone is infected with plasmodium
14:47
vivax, the first priority is to
14:49
eliminate the parasites that are
14:51
actively multiplying in their
14:53
bloodstream. This is called blood stage
14:56
treatment and it's our first line of
14:58
defense against malaria symptoms. To
15:00
understand blood stage treatment, we
15:02
need to see what's happening inside red
15:04
blood cells during a vivax infection.
15:07
The parasites go through several stages
15:10
as they multiply and eventually burst
15:12
out to infect new cells. Here we can see
15:14
the parasites journey inside a red blood
15:17
cell. It starts as a ring-shaped form,
15:19
grows into a trophoid, then develops
15:21
into a schisant that eventually bursts
15:24
to release new parasites called
15:25
mirazoids. This cycle repeats every 48
15:29
hours in vivac malaria.
15:31
The primary weapon against these
15:33
bloodstage parasites is chlorocqueen.
15:36
This drug has been the gold standard for
15:37
treating vivac malaria for decades
15:40
because it's effective, affordable, and
15:42
generally well tolerated. Chloricquin
15:45
works by interfering with the parasites
15:47
ability to detoxify harmful waste
15:49
products. When parasites digest
15:52
hemoglobin from red blood cells, they
15:54
produce toxic heem. Chloricquin prevents
15:57
them from safely disposing of this heem,
16:00
essentially poisoning the parasite.
16:02
However, we now have a significant
16:03
problem. In many parts of the world,
16:06
plasmodium vivax has developed
16:08
resistance to chlorocqueen. This means
16:10
the drug no longer works effectively
16:12
against these resistant strains. When
16:15
chloricquin resistance is suspected or
16:17
confirmed, doctors turn to artemcanin
16:19
based combination therapies known as
16:21
acts. These are more complex treatments
16:24
that combine arteesin derivatives with
16:26
other antimmalarial drugs. Let's look at
16:29
how antimmalarial drugs are classified
16:31
based on their targets and goals. This
16:34
helps us understand why different drugs
16:36
are used for different purposes in
16:38
malaria treatment. This table shows the
16:40
three main categories of antimmalarial
16:43
drugs. Blood schizonttoicides like
16:45
chloricquin and AC target the parasites
16:48
in red blood cells. Tissue skizonticides
16:50
target liver stages and gatocytoal drugs
16:54
prevent transmission by killing the
16:55
sexual forms of the parasite. The key
16:58
takeaway is that blood stage treatment
17:00
is crucial but not sufficient on its
17:02
own. While chlorocquin remains effective
17:04
in many areas, healthcare providers must
17:07
be aware of resistance patterns and be
17:09
ready to use ACTs when needed. This
17:12
targeted approach helps clear the
17:14
immediate infection and reduce symptoms.
17:16
While treating the bloodstage infection
17:19
helps with immediate symptoms, it
17:21
doesn't solve the complete problem. The
17:23
hypnosit sleeping in the liver will
17:25
eventually wake up and cause relapses.
17:28
These dormant hypnosits in the liver are
17:30
like ticking time bombs. They can
17:32
reactivate weeks or months later causing
17:35
new episodes of malaria even after the
17:37
patient feels completely recovered.
17:41
This is why we need what's called a
17:43
radical cure. Unlike partial treatment
17:45
that only targets bloodstage parasites,
17:48
radical cure eliminates both the
17:50
bloodstage infection and the dormant
17:52
liver stage hypnosits.
17:54
Two main drugs can achieve radical cure.
17:58
Primacqueen has been the gold standard
17:59
for decades, requiring a 14-day
18:01
treatment course. Tofenqueen is a newer
18:04
option that offers the advantage of
18:06
single dose treatment, which greatly
18:08
improves patient compliance.
18:12
Modern research has developed ways to
18:14
detect hypnos infections through
18:16
antibbody testing. This helps doctors
18:19
identify patients who have dormant
18:20
parasites in their liver and need
18:22
radical cure treatment.
18:25
The key takeaway is that radical cure is
18:28
absolutely essential for complete pivax
18:31
treatment. Without eliminating the
18:32
hypnosits in the liver, patients will
18:34
continue to experience relapses. Only
18:37
Primocqueen and Tphenoquin can achieve
18:39
this complete eradication of the
18:41
parasite.
18:42
Before we can safely use Primacqueen or
18:45
Tofphenquin for radical cure, there's a
18:47
critical safety consideration we must
18:49
address. G6PD deficiency. G6PD
18:53
deficiency is a genetic condition that
18:55
affects red blood cells. It's caused by
18:58
a deficiency in the glucose 6 phosphate
19:00
dehydrogenase enzyme. This condition
19:02
affects about 400 million people
19:04
worldwide and is more common in males
19:07
due to XL inheritance.
19:10
In normal conditions, the G6PD enzyme
19:12
plays a crucial role in protecting red
19:14
blood cells. It converts glucose 6
19:17
phosphate to six phosphogglycerate
19:19
producing NADPH in the process. This
19:22
NADPH then works with glutathione to
19:24
protect red blood cell membranes from
19:26
oxidative damage. In people with G6PD
19:30
deficiency, NADPH production is reduced,
19:33
making red blood cells vulnerable to
19:35
oxidative stress. When primocqueen or
19:37
tephenocqueen are given to these
19:39
patients, the drugs cause oxidative
19:41
damage that can lead to severe
19:43
hemolysis, the destruction of red blood
19:45
cells. This diagram shows what happens
19:48
at the cellular level. Oxidative stress
19:50
causes hemoglobin to denature forming
19:53
hines bodies inside the red blood cells.
19:56
These hines bodies damage the cell
19:58
membrane making the cells targets for
20:00
destruction by macrofasages in the
20:02
spleen. This results in bite cells and
20:04
spherosittes leading to severe anemia.
20:08
This is why testing for G6PD deficiency
20:11
is absolutely essential before giving
20:13
primacquine or tphenocquin. All patients
20:16
must be tested preferably with
20:17
quantitative G6PD testing. For patients
20:20
who are G6PD deficient, alternative
20:23
treatments must be used to prevent
20:25
life-threatening hemolysis.
20:28
The key takeaway is this. G6PD testing
20:31
before radical cure is not optional.
20:34
It's a life-saving safety requirement.
20:36
This simple test ensures that we can
20:38
provide safe and effective treatment for
20:40
all patients with vivax malaria.
20:44
Drug resistance is becoming a serious
20:46
challenge in treating plasmodium vivac
20:49
malaria. When parasites develop
20:51
resistance, medications that once worked
20:54
effectively become less powerful or
20:56
completely ineffective. Normally
20:58
antimmalarial drugs like chloricqueen
21:00
work by attacking the parasite and
21:02
preventing it from multiplying in the
21:04
bloodstream.
21:06
However, when parasites develop
21:08
resistance, they can survive even when
21:10
exposed to the drug. The medication
21:12
becomes ineffective and the infection
21:15
continues.
21:16
Chloricquin was once the gold standard
21:18
treatment for pivax malaria. For
21:21
decades, it was highly effective and
21:23
widely used around the world. However,
21:25
starting in the early 2000s, reports
21:28
began emerging of Pivax parasites that
21:30
could survive chloricquin treatment.
21:33
This was first documented in Papua New
21:36
Guinea and Indonesia. Today, chloricquin
21:38
resistance in Pivax has spread to many
21:41
regions, making treatment much more
21:43
challenging and requiring alternative
21:45
medications.
21:47
Chloricquin resistance in Pivax is not
21:49
evenly distributed around the world.
21:51
It's most commonly found in Southeast
21:53
Asia, including Indonesia, Papua New
21:56
Guinea, and parts of the Solomon
21:57
Islands.
21:59
Resistance has also been reported in
22:01
parts of South America, particularly in
22:03
areas with high malaria transmission
22:05
rates. The Pacific region, especially
22:08
Papio New Guinea, was among the first
22:10
places where chloricquin resistant Pivax
22:13
was documented.
22:15
Drug resistance has significantly
22:17
complicated Pivax treatment. In the
22:20
past, doctors could rely on chloricquin
22:22
as a simple, effective, and inexpensive
22:24
treatment option. Now, in areas with
22:26
chloricquin resistance, healthcare
22:28
providers must use alternative drugs,
22:31
follow more complex treatment protocols,
22:33
and deal with higher medication costs.
22:36
Scientists and researchers around the
22:38
world are working hard to develop new
22:40
antimmalarial drugs that can overcome
22:43
resistance. This involves a complex
22:46
pipeline from initial discovery to final
22:48
approval.
22:50
Drug resistance represents a significant
22:52
challenge in the fight against Pivvax
22:54
malaria. As resistance spreads, we need
22:57
continued research and development of
22:59
new treatments to stay ahead of this
23:01
evolving threat.
23:03
Understanding and addressing drug
23:05
resistance is crucial for effective
23:07
malaria control and eventual elimination
23:09
efforts worldwide. Preventing mosquito
23:12
bites is the most effective way to
23:14
prevent malaria transmission. There are
23:17
two main approaches, personal protection
23:19
and environmental control. Personal
23:22
protection involves creating barriers
23:24
between you and mosquitoes. Let's
23:27
explore the three main methods that have
23:29
proven most effective. First, wearing
23:32
long sleeves and pants provides a
23:34
physical barrier against mosquito bites.
23:36
Light colored clothing is preferred as
23:38
mosquitoes are attracted to dark colors.
23:41
This protection is especially important
23:43
during dawn and dusk when mosquitoes are
23:46
most active.
23:48
Second, mosquito repellents containing
23:50
de are highly effective at preventing
23:52
bites. Apply repellent to all exposed
23:55
skin and clothing and remember to
23:57
reapply every 4 to 6 hours for continued
24:00
protection.
24:02
Third, insecticide treated bed nets are
24:04
considered the most effective prevention
24:06
method. They provide a physical barrier
24:09
while you sleep, and the insecticide
24:11
kills mosquitoes that come into contact
24:13
with the net.
24:16
Environmental control focuses on
24:18
reducing mosquito populations by
24:20
eliminating their breeding sites.
24:22
Mosquitoes need standing water to
24:24
reproduce, so removing these sources is
24:26
crucial. Mosquitoes can breed in
24:28
surprisingly small amounts of water.
24:31
Common breeding sites include flower
24:33
pots, clogged gutters, old tires, and
24:36
any container that can hold water for
24:38
more than a week. To eliminate breeding
24:41
sites, empty all containers at least
24:43
weekly. Keep gutters clean, cover water
24:45
storage tanks, and remove any
24:47
unnecessary items that can collect
24:49
water. Even small actions can
24:52
significantly reduce mosquito
24:53
populations. Remember, the most
24:57
effective approach combines personal
24:59
protection with environmental control.
25:02
Consistency in applying these methods
25:04
and communitywide participation greatly
25:06
increases their effectiveness in
25:08
preventing malaria transmission. When
25:11
traveling to areas where plasmodium
25:13
vivax malaria is common, taking
25:15
preventive medication called prophylaxis
25:17
can protect you from infection.
25:20
Think of it as building a protective
25:22
shield before you encounter the
25:24
parasite. Prophylaxis means taking
25:26
medication before you get sick to
25:28
prevent the disease from occurring. It's
25:30
like wearing a seat belt. You put it on
25:33
before you need it, not after an
25:35
accident happens. Your doctor will
25:37
recommend prophylaxis if you're
25:39
traveling to areas where malaria is
25:41
common, especially tropical and
25:43
subtropical regions. This includes parts
25:45
of Africa, Asia, Central, and South
25:48
America, and some Pacific islands. The
25:51
timing of prophylactic medication is
25:53
crucial. You typically start taking the
25:55
medication one to two weeks before
25:57
travel, continue throughout your entire
26:00
trip, and keep taking it for several
26:02
weeks after you return home. Common
26:05
prophylactic medications for vivax
26:07
malaria include chloricquin, doxycyc,
26:10
autoquinone, progil, and mephloquin.
26:13
Your doctor will choose the best option
26:15
based on your destination, medical
26:17
history, and potential drug resistance
26:19
in the area. Here's how prophylaxis
26:21
works in the malaria life cycle. The
26:23
medications target the parasite at
26:25
different stages, preventing it from
26:27
establishing infection in your liver and
26:30
bloodstream. This breaks the cycle
26:32
before symptoms can develop. Remember
26:35
these key points about malaria
26:36
prophylaxis. Start before travel, take
26:40
consistently during your trip, and
26:42
complete the full course after
26:44
returning. Always consult your doctor
26:46
for personalized recommendations based
26:48
on your specific travel plans and health
26:50
status. The relationship between P Vivax
26:54
and the Duffy antigen is a fascinating
26:56
example of how genetics can protect
26:58
against infectious disease.
27:00
Understanding this connection helps
27:02
explain why malaria patterns differ
27:04
around the world. The Duffy antigen is a
27:07
protein found on the surface of red
27:08
blood cells. For Pivax parasites, this
27:12
this antigen acts like a key that
27:14
unlocks the door to enter and infect red
27:16
blood cells. When Pivax measoes are
27:18
released into the bloodstream, they
27:21
specifically seek out red blood cells
27:23
that have the Duffy antigen. The
27:25
parasite binds to this antigen like a
27:27
lock and key mechanism. Here's where
27:29
genetics becomes protective. Many
27:32
people, especially in West Africa, are
27:34
Duffy negative, meaning they lack the
27:36
Duffy antigen on their red blood cells.
27:38
Without this receptor, Pivax cannot
27:41
invade their cells. This genetic
27:43
protection explains a major geographic
27:46
pattern in malaria. Pivax is much less
27:49
common in Africa compared to Asia, the
27:51
Americas, and other regions where most
27:53
people are Duffy positive. However,
27:55
recent research has uncovered something
27:57
surprising. There have been rare
27:59
documented cases of Pivax infection in
28:02
people who are Duffy negative. This
28:04
discovery has opened up new questions
28:06
for scientists. Understanding the Duffy
28:09
antigen connection has important
28:11
implications.
28:13
It helps explain malaria distribution
28:15
patterns, guides treatment strategies,
28:17
and shows how human genetic diversity
28:20
can provide natural protection against
28:22
infectious diseases. Developing a
28:24
vaccine against plasmodium vivax has
28:26
been one of the most challenging goals
28:28
in malaria research. Unlike other
28:30
diseases, pivax presents unique
28:33
obstacles that scientists are now
28:35
beginning to overcome. The challenge
28:37
lies in Pivax's complex life cycle. A
28:41
successful vaccine must target multiple
28:43
stages from the initial infection in the
28:45
liver to the blood stage parasites that
28:48
cause symptoms. Scientists are
28:50
developing what's called a multivalent
28:52
multi-stage vaccine. This means the
28:55
vaccine contains components that can
28:58
attack the parasite at different points
28:59
in its life cycle, providing broader
29:02
protection. Several promising vaccine
29:04
candidates are now in clinical trials.
29:06
These vaccines use different approaches.
29:09
Some focus on preventing infection while
29:11
others aim to reduce disease severity or
29:14
block transmission to mosquitoes.
29:16
The key breakthrough is targeting
29:18
functionally conserved epitopes, parts
29:20
of the parasite that remain the same
29:22
across different strains. This approach
29:25
aims to create broadly neutralizing
29:27
immunity that works against multiple
29:29
pivax variants.
29:32
While we don't have an approved pivax
29:34
vaccine yet, the progress is
29:36
encouraging. Researchers expect that
29:38
within the next decade, we may see the
29:40
first effective vaccines that can
29:42
significantly reduce pivax infections
29:45
and help with elimination efforts.
29:48
Malaria elimination represents one of
29:50
the most ambitious global health goals
29:52
of our time. Countries around the world
29:55
are implementing comprehensive
29:56
strategies to completely stop malaria
29:59
transmission within their borders.
30:01
Elimination requires a multifaceted
30:04
approach. Countries must simultaneously
30:06
tackle vector control, improve
30:08
diagnostic capabilities, ensure
30:11
effective treatment and address
30:12
underlying social and environmental
30:14
factors that contribute to malaria
30:16
transmission. Sri Lanka stands as one of
30:19
the most remarkable success stories in
30:21
malaria elimination. After decades of
30:24
endemic malaria, the country achieved
30:26
elimination in 2016 through sustained
30:29
political commitment and comprehensive
30:31
control measures. China represents
30:34
another major elimination success
30:37
through massive coordinated efforts
30:38
involving improved case management,
30:41
vector control and crossber
30:43
collaboration. China eliminated malaria
30:46
in 2021, becoming the first country in
30:48
the western Pacific region to achieve
30:50
this milestone in over three decades.
30:53
The timeline of global malaria control
30:56
shows remarkable progress over the
30:58
decades. From the early control efforts
31:00
in the 1950s to modern elimination
31:02
programs, we can see how sustained
31:05
efforts and improved strategies have
31:07
dramatically reduced malaria incidents
31:09
worldwide.
31:11
Many other countries are making
31:12
significant progress toward elimination.
31:14
Nepal aims to eliminate malaria by 2025
31:18
while the greater Mikong sub region
31:20
countries are working together through
31:22
the Mikong malaria elimination program
31:24
to achieve elimination by 2030. The key
31:28
takeaway is that malaria elimination is
31:30
achievable but it requires sustained
31:33
commitment, comprehensive strategies and
31:35
international cooperation. Success
31:38
stories like Sri Lanka and China prove
31:40
that with the right approach, even
31:42
countries with long histories of endemic
31:44
malaria can achieve elimination in the
31:47
fight against plasmodium vivax malaria.
31:49
Regional coordination is essential. The
31:52
Asia-Pacific malaria elimination network
31:55
known as 8men plays a crucial leadership
31:57
role in this effort. APMEN is a network
32:00
of countries across the Asia-Pacific
32:02
region working together to eliminate
32:04
malaria. Within 8MEN, there's a
32:07
specialized group called the Vivvax
32:09
working group that focuses specifically
32:10
on P Vivvax challenges. The ATM vivax
32:13
working group has three main
32:15
responsibilities. First, they build the
32:18
evidence base for radical cure
32:20
treatments. This means conducting
32:22
research and gathering data to prove
32:24
which treatments work best. Second, they
32:26
support policy changes to incorporate
32:28
radical cure into national treatment
32:31
strategies.
32:32
This involves working with governments
32:34
to update their malaria treatment
32:36
guidelines based on the latest evidence.
32:38
Third, they coordinate elimination
32:40
efforts across the entire Asia-Pacific
32:43
region. This means ensuring countries
32:45
work together, share information, and
32:47
align their strategies to eliminate
32:49
pivax malaria. The importance of Apen's
32:52
work cannot be overstated. PVA malaria
32:55
is particularly challenging because of
32:58
its ability to hide in the liver and
33:00
cause relapses. Regional coordination
33:02
ensures that elimination efforts are
33:04
comprehensive and effective through
33:06
evidence-based research, policy support,
33:08
and regional coordination. APMAN's
33:10
Vivvax working group is leading the
33:12
charge toward Pivax elimination in one
33:15
of the world's most affected regions.
33:18
Malaria elimination efforts face a
33:20
particularly stubborn opponent in
33:21
plasmodium vivac. Experts worldwide
33:24
agree that Pivax will likely be the very
33:27
last human malaria parasite species to
33:29
be completely eliminated from our
33:31
planet. This challenge stems from three
33:34
main categories of obstacles that make
33:36
PIVAX uniquely difficult to eliminate.
33:38
Its complex biology, limitations in
33:41
available treatments, and difficulties
33:43
in detection and diagnosis. The biggest
33:46
biological challenge is the hypnosid
33:48
stage. These dormant forms hide in the
33:51
liver and can reactivate weeks or months
33:54
after the initial infection, causing
33:56
relapses. They're completely invisible
33:58
to standard diagnostic tests, making it
34:00
impossible to know if someone is truly
34:02
cured. Treatment presents its own set of
34:05
barriers. To achieve a radical cure that
34:08
eliminates hypnosids, patients need
34:11
eight aminoquinolene drugs like
34:13
primocqueen. However, these drugs can be
34:15
dangerous for people with G6PD
34:17
deficiency, a common genetic condition.
34:20
Additionally, we're seeing growing drug
34:22
resistance and treatment courses are
34:24
long and difficult to complete.
34:26
Detection and diagnosis face significant
34:29
hurdles. Pivax typically maintains lower
34:32
parasite levels in the blood, making it
34:34
harder to detect. Many infections are
34:37
completely asymptomatic and recent
34:39
research suggests the parasite can hide
34:41
in cryptic reservoirs like the spleen
34:43
and bone marrow. Most concerning
34:46
transmission to mosquitoes can occur
34:47
even before symptoms appear. Despite
34:50
these formidable challenges, elimination
34:53
is not impossible. Success will require
34:56
innovative drug development to replace
34:58
current treatments, better diagnostic
35:00
tools that can detect hidden infections,
35:02
effective vaccines, and most
35:04
importantly, sustained global commitment
35:07
to integrated elimination strategies.
35:09
The fight against Pivax will be long,
35:12
but with continued research and
35:14
international cooperation, we can
35:16
eventually overcome even the most
35:18
persistent malaria parasite. Recent
35:20
research has brought new insights into
35:22
the use of Primacqueen in breastfeeding
35:24
women, challenging existing guidelines
35:27
and opening new possibilities for
35:29
malaria treatment.
35:31
Traditionally, the World Health
35:32
Organization has recommended avoiding
35:34
Primacqueen in breastfeeding women due
35:36
to concerns about potential risks to the
35:38
infant, particularly those with G6PD
35:42
deficiency.
35:44
Recent clinical data and sophisticated
35:46
modeling studies have revealed that the
35:48
benefits of Premacqueen treatment in
35:50
breastfeeding women may actually
35:52
outweigh the potential risks. These
35:55
studies show improved maternal health
35:57
outcomes and reduced malaria
35:59
transmission.
36:01
The new research suggests that when we
36:03
carefully weigh the risks against the
36:05
benefits, the scale tips in favor of
36:08
treatment. The benefits of preventing
36:10
malaria relapses and protecting maternal
36:13
health appear to outweigh the potential
36:15
risks to the infant.
36:18
This research is particularly important
36:20
because breastfeeding provides numerous
36:23
documented health benefits for both
36:24
mothers and babies.
36:27
The challenge has been balancing these
36:29
benefits with the need for effective
36:31
malaria treatment. Based on this
36:33
emerging evidence, medical experts and
36:35
researchers are calling for a
36:37
re-examination of current WH
36:39
recommendations. They advocate for an
36:42
evidence-based approach that considers
36:43
individual risk assessment rather than
36:46
blanket restrictions.
36:49
This remains an evolving area of
36:51
research where new evidence continues to
36:54
emerge. As more clinical data becomes
36:56
available, treatment guidelines may be
36:59
updated to reflect the latest scientific
37:02
understanding. Healthcare providers
37:04
should stay informed about these
37:05
developments to provide the best care
37:08
for their patients. The future of
37:09
plasmodium vivax research is focused on
37:12
developing breakthrough solutions to
37:14
finally eliminate this persistent
37:16
parasite. Scientists worldwide are
37:19
working on multiple fronts to overcome
37:21
the unique challenges that Pivax
37:23
presents. Drug development research is
37:26
prioritizing new compounds that can
37:28
effectively target the dormant hypnosid
37:30
stage in the liver. Current efforts
37:33
focus on improving upon prim with safer,
37:35
more effective alternatives that don't
37:37
require G6PD testing.
37:40
Vaccine research is advancing with
37:42
multi-stage approaches that target
37:44
different phases of the parasites life
37:46
cycle. Scientists are developing
37:49
vaccines that can prevent both initial
37:51
infection and relapses by targeting
37:53
multiple parasite antigens
37:55
simultaneously.
37:57
Diagnostic research aims to develop
37:59
rapid, accurate tests that can be used
38:01
in remote field settings. These new
38:04
tools will help detect low-level
38:05
infections and distinguish between
38:08
different plasmodium species more
38:09
effectively.
38:11
Understanding the parasites biology is
38:13
crucial for developing effective
38:15
interventions. research focuses on how
38:17
hypnosits remain dormant, how drug
38:19
resistance develops, and what triggers
38:22
relapses after months of dormcancy.
38:25
Transmission dynamics research helps
38:27
scientists understand how Pivax spreads
38:30
in different populations and
38:31
environments. This knowledge is
38:33
essential for designing targeted
38:35
elimination strategies and predicting
38:37
where outbreaks might occur. The
38:40
ultimate goal of all this research is
38:42
complete elimination of pivax. By
38:45
integrating advances in drugs, vaccines,
38:47
diagnostics, and our understanding of
38:49
the parasite, scientists aim to develop
38:52
comprehensive strategies that can
38:54
finally eradicate this persistent threat
38:56
to global health. We've completed our
38:59
comprehensive journey through plasmodium
39:01
vivac. Now, let's summarize the most
39:03
important points you need to remember
39:05
about this significant malaria parasite.
39:08
First and most importantly, plasmodium
39:10
vivax has an incredibly complex life
39:13
cycle that involves both mosquitoes and
39:15
humans. Understanding this cycle is
39:18
crucial because it explains why vivvax
39:20
malaria is so persistent and difficult
39:22
to eliminate. Second, plasmodium vivax
39:26
is a major global health threat
39:27
affecting over a third of the world's
39:29
population. With 4.5 million cases in
39:33
2020 alone, it's the most widespread
39:35
cause of recurring malaria worldwide.
39:38
Third, treating vivax malaria requires a
39:40
two-pronged approach. We must target
39:43
both the bloodstage parasites causing
39:45
symptoms and the dormant liver stage
39:47
hypnosits to prevent relapses. This
39:49
radical cure is essential but
39:51
complicated by drug resistance and
39:53
genetic factors. Fourth, prevention
39:56
remains our most powerful tool against
39:58
vivax malaria. Vector control through
40:01
bed nets, indoor spraying, and
40:03
environmental management combined with
40:05
prophylactic medications for travelers
40:07
can dramatically reduce transmission.
40:10
Finally, the future holds promise for
40:12
vivac malaria control. New vaccines are
40:15
in development, elimination programs are
40:18
showing success in several countries,
40:20
and research continues to improve our
40:22
understanding and treatment options.
40:24
Understanding plasmodium vivax is
40:26
crucial for global health. By learning
40:29
about its complex biology, treatment
40:31
challenges, and prevention strategies,
40:33
we're better equipped to fight this
40:35
persistent parasite.
40:37
Thank you for joining us on this
40:38
educational journey through the world of
40:40
Vivvax malaria.
#Infectious Diseases
#Public Health
#Biological Sciences