Up next in 10

The Life Cycle of Plasmodium vivax - Malaria Explained
Website: https://biologynotesonline.com/
Facebook: https://www.facebook.com/biologynotesonline
Instagram: https://www.instagram.com/biologynotesonline/?hl=en
Show More Show Less View Video Transcript
0:00
Plasmodium vivax is a microscopic
0:02
single-sellled parasite that causes one
0:04
of the most common forms of malaria
0:06
worldwide. Think of it as a tiny
0:08
mischievous traveler that has learned to
0:11
survive by living inside other
0:12
organisms. Under a microscope, we can
0:15
actually see these parasites hiding
0:17
inside our blood cells.
0:20
Plasmodium vivax belongs to a family of
0:22
parasites that cause malaria. There are
0:25
actually five different species that can
0:27
infect humans, but Pivax is one of the
0:30
most widespread. While Pivax is
0:32
generally considered less dangerous than
0:34
its cousin Palsaparum,
0:36
don't let that fool you. It can still
0:38
make you very sick and cause serious
0:41
complications.
0:43
Pivax has a massive global reach. About
0:45
2.5 billion people worldwide are at risk
0:48
of infection. Unlike palsiparum which is
0:51
concentrated in Africa, pivox thrives in
0:53
many regions outside of Africa. What
0:56
makes pivox particularly tricky is that
0:59
it can survive in cooler temperatures
1:01
than other malaria parasites. This
1:03
allows it to spread to temperate regions
1:06
and makes it a persistent global health
1:08
challenge. So remember, pivox may be
1:11
small, but it's a formidable opponent
1:13
that affects billions of people
1:15
worldwide. Understanding this parasite
1:17
is the first step in learning how to
1:19
fight it effectively.
1:22
Plasmodium vivax has a very specific way
1:24
of getting from one person to another.
1:27
It cannot spread through the air, water,
1:29
or direct contact between people.
1:31
Instead, it relies entirely on a
1:34
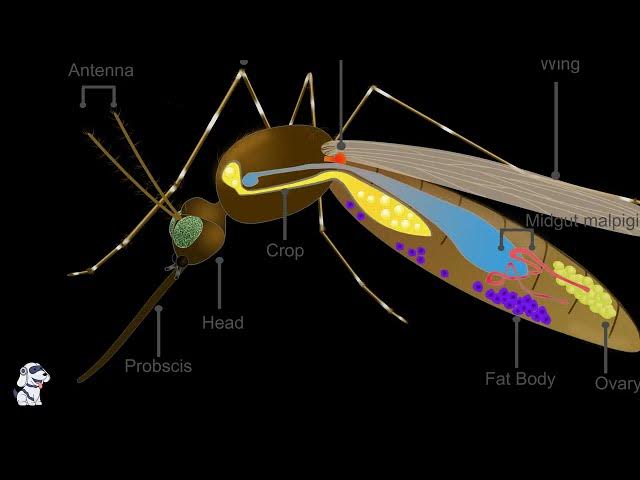
particular type of mosquito. Female
1:36
anophles mosquitoes are the exclusive
1:38
vectors for plasmodium vivac. These
1:40
mosquitoes are the only way this
1:42
parasite can travel from one human to
1:44
another. No mosquito, no transmission.
1:48
When an infected female Anophles
1:50
mosquito bites a human, she injects
1:52
saliva containing plasmodium vivac
1:55
parasites directly into the bloodstream.
1:57
This is the moment of transmission. The
1:59
parasite hitches a ride from the
2:01
mosquito into its new human host.
2:05
Here's how the transmission works. The
2:08
infected mosquito contains plasmodium
2:10
vivax parasites in its salivary glands.
2:13
When it bites, these parasites are
2:15
injected into the human bloodstream
2:17
along with the mosquito's saliva. During
2:19
the bite, the parasites travel from the
2:21
mosquito into the human host. This
2:24
transfer happens in seconds, but it
2:26
starts a complex infection cycle that
2:28
can last for years.
2:31
This is crucial to understand.
2:32
Plasmodium vivax cannot spread directly
2:35
from person to person through the air or
2:37
through contaminated water. The anophles
2:40
mosquito is the absolute requirement for
2:42
transmission. This makes mosquito
2:44
control a critical strategy in fighting
2:47
malaria.
2:50
Since mosquitoes are the only way
2:52
plasmodium vivax spreads, controlling
2:54
mosquito populations is extremely
2:56
effective. Bed nets, insecticides,
2:59
removing standing water, and indoor
3:00
spraying all help break the transmission
3:03
cycle. No mosquitoes means no new
3:05
infections. Remember, breaking the
3:08
mosquito transmission cycle is the key
3:10
to stopping plasmodium vivac spread.
3:13
This simple biological fact makes
3:14
mosquito control one of our most
3:16
powerful tools against malaria.
3:20
Once inside you, plasmodium vivac starts
3:22
its asexual cycle. But what does asexual
3:25
reproduction actually mean? The
3:27
infection begins when an infected
3:29
mosquito bites you and injects sporzoits
3:31
directly into your bloodstream. These
3:34
sporzoids are like tiny travelers
3:36
searching for a new home. They move
3:38
through your bloodstream with a specific
3:40
destination in mind. Let's look at what
3:42
these sporzoids actually look like and
3:45
understand their structure better.
3:49
This marks the beginning of the asexual
3:51
cycle inside your body. The sporzoids
3:54
are now ready to find their target
3:55
destination and begin the next phase of
3:58
infection. After the mosquito bite, the
4:01
sporzoids don't just wander around
4:02
aimlessly. They have a very specific
4:05
destination in mind, your liver. These
4:08
tiny parasites travel through your
4:10
bloodstream like guided missiles heading
4:13
straight for the liver. The liver is
4:16
their target because it provides the
4:18
perfect environment for what they need
4:20
to do next. The liver contains millions
4:22
of cells called hpatocytes. These are
4:25
large specialized cells that perform
4:28
many important functions for your body.
4:30
Here's what a hpatocite looks like up
4:32
close.
4:33
These cells are packed with organels and
4:36
have an irregular shape that gives them
4:38
a large surface area for their many
4:40
functions. Now comes the invasion. The
4:43
sporzoids don't just bump into the
4:44
hpatocytes. They actively penetrate and
4:47
enter these liver cells. Think of it
4:50
like the parasite checking into a hotel
4:52
for an extended stay.
4:54
This microscopic view shows what
4:56
infected liver cells look like. Once
4:59
inside the hpatocytes, the sporzoits
5:01
have found their perfect home, a safe,
5:03
nutrient-rich environment where they can
5:05
begin to multiply and grow. Just like
5:08
hotel guests settling into their rooms,
5:10
the sporzoites make themselves
5:12
comfortable inside the hpatocytes.
5:15
They have everything they need.
5:17
Protection from your immune system and
5:19
plenty of resources to fuel their next
5:21
phase of development.
5:23
This liver stage is crucial for the
5:25
parasites life cycle. Inside these
5:27
hpatocytes, the sporosoids will
5:30
transform and multiply dramatically,
5:32
preparing for their next move into your
5:34
bloodstream.
5:36
Once sporzoids successfully invade liver
5:38
cells, they begin an incredible
5:41
transformation process called liver
5:43
schizogy. This is where the real
5:45
multiplication magic happens. Here we
5:48
can see the progression inside a liver
5:50
cell. The sporzoid that entered the
5:52
liver cell begins to transform and
5:54
develop into what we call a skits.
5:58
Think of the infected liver cell as a
6:00
microscopic factory. Initially, there's
6:03
just one sporzoid inside the liver cell,
6:05
but this single parasite is about to
6:07
become incredibly productive. The sporzo
6:10
transforms into a skisant, which is
6:13
essentially a parasite factory. The
6:15
skisant grows larger and begins the
6:17
process of creating many new parasites
6:20
through asexual reproduction inside the
6:22
skits. Rapid multiplication occurs. A
6:25
single sporzoid can produce thousands of
6:27
new parasites called meazoids. This
6:30
process typically takes 6 to 15 days in
6:32
plasmodium vivax. The numbers are
6:34
staggering. From just one sporzoid, a
6:37
single schizont,000
6:40
to 30,000 meazoids. This massive
6:43
multiplication is what makes malaria
6:45
such a formidable infection.
6:47
During liver skisogy, the skis underos
6:50
dramatic changes. It grows significantly
6:53
in size, develops complex internal
6:55
structures and organizes itself to
6:58
efficiently produce and eventually
6:59
release thousands of measoids.
7:02
The key takeaway is that liver schizogy
7:05
represents the critical amplification
7:07
stage of plasmodium vivax infection.
7:10
This is where the parasite transforms
7:12
from a single invader into thousands of
7:14
infectious agents, setting the stage for
7:16
the massive blood infection that
7:18
follows. After this intensive
7:21
multiplication period in the liver, the
7:23
mature scadzant is ready to release its
7:25
army of meroszoids into the bloodstream
7:28
where the next phase of the infection
7:29
will begin.
7:31
Now we encounter one of the most
7:33
challenging aspects of plasmodium vivac,
7:35
the formation of hypnosits. These are
7:38
special dormant forms that make this
7:40
parasite particularly tricky to
7:41
eliminate. When sporzoids enter the
7:44
liver, most develop normally and
7:46
continue the life cycle. However, some
7:48
sporzoids take a different path. They
7:51
transform into hypnosits, which are
7:53
dormant, inactive forms. Think of
7:55
hypnosits as sleeping agents hidden in
7:57
your liver. They can remain completely
8:00
inactive and undetectable for weeks,
8:02
months, or even years. This dormcy
8:05
period varies greatly between
8:07
individuals and geographic strains of
8:08
the parasite. The real problem with
8:11
hypnosits is that they can suddenly
8:13
react without warning. When they wake
8:16
up, they begin developing normally,
8:19
releasing meroszoids into the
8:20
bloodstream and causing a malaria
8:22
relapse, even months or years after the
8:25
initial infection was treated. This
8:27
dormant stage is what makes plasmodium
8:30
vivac so persistent and difficult to
8:32
eliminate. Standard antimmalarial drugs
8:35
can clear the active parasites from the
8:37
blood, but they cannot reach the
8:39
sleeping hypnosites hidden in the liver.
8:42
This is why people can experience
8:44
multiple episodes of malaria from a
8:46
single mosquito bite. Understanding
8:48
hypnosits is crucial because they
8:50
represent the hidden reservoir that
8:52
keeps vivac malaria circulating in
8:54
populations. They are the reason why
8:57
eliminating this form of malaria
8:59
requires special treatment strategies
9:01
that can target both active parasites
9:03
and these dormant forms. After spending
9:06
time multiplying in the liver, the
9:08
parasites are ready for their next big
9:10
move. The liver skisants have grown full
9:13
of new parasites called morzoids. And
9:16
now it's time for them to break free.
9:18
Inside each liver cell, the skezant has
9:21
been busy creating dozens of new
9:23
moroids. Think of it like a factory
9:26
that's been working overtime and now the
9:28
warehouse is completely full of finished
9:30
products. As more and more mezzoids pack
9:32
into the skids, pressure builds up
9:35
inside the liver cell. The cell membrane
9:38
can't contain all these parasites much
9:40
longer. Then it happens. The skids
9:43
bursts open. The liver cell membrane
9:45
ruptures and all those mezzoids are
9:47
suddenly released into the bloodstream.
9:50
It's like a graduation ceremony where
9:52
all the parasites leave school at once.
9:55
The newly released mezzoids now flow
9:57
through the bloodstream. Each morazzo is
10:00
a tiny mobile parasite equipped with
10:03
everything it needs to find and invade
10:05
red blood cells. Now let's take a closer
10:07
look at what these mezzoids are designed
10:09
to do. This detailed view shows exactly
10:12
how a mezzoid will invade a red blood
10:15
cell. The mezzoid invasion process is
10:17
incredibly sophisticated. First, the
10:20
morzoid attaches to a red blood cell,
10:22
then reorients itself and forms a
10:24
junction. It then pushes its way inside
10:27
and creates a protective vacule where it
10:29
can safely develop. Here's what the
10:31
bloodstream looks like under a
10:33
microscope after mezoids have been
10:35
released. You can see the normal red
10:38
blood cells and some that have already
10:40
been invaded by parasites. The key
10:42
takeaway is that this moment represents
10:44
a critical transition in the parasites
10:46
life cycle. The morosoites have
10:49
graduated from their liver stage and are
10:51
now ready to begin the blood stage of
10:53
infection where they'll invade red blood
10:55
cells and cause the symptoms of malaria.
10:59
This release of mezoites into the
11:01
bloodstream is like opening the
11:03
floodgates. What started as a small
11:05
infection in the liver now becomes a
11:08
systemic infection that will affect the
11:10
entire circulatory system. Now we enter
11:12
the blood stage of the plasmodium vivax
11:15
life cycle. The morzoids that were
11:18
released from the liver are now
11:19
circulating in the bloodstream ready to
11:21
invade red blood cells. Mirazoids
11:24
specifically target reticulosytes which
11:26
are immature red blood cells. These
11:29
young cells are preferred because they
11:31
contain the ribosomes and other cellular
11:33
machinery that the parasite needs to
11:35
survive and multiply. Watch as the
11:38
morazzo move through the bloodstream and
11:40
invade the reticulosytes.
11:42
This invasion process is rapid and
11:44
efficient. Once inside the reticular
11:46
site, the mezzoid begins to transform.
11:49
This process is called ariththroitic
11:51
schizogy, which means asexual
11:53
reproduction within red blood cells.
11:56
First, the mezzoid develops into a
11:58
trophoid. The trophoid is the feeding
12:01
stage of the parasite. It consumes the
12:03
hemoglobin inside the red blood cell,
12:06
growing larger and more active. As the
12:08
trophoid feeds and grows, it eventually
12:10
transforms into a skisant. The skisant
12:14
is the reproductive stage where the
12:15
parasite divides to create multiple new
12:17
mezzoids. Inside the schizont, multiple
12:20
new mezzoids are formed through asexual
12:23
reproduction. When the schizont is
12:25
mature, it ruptures the red blood cell,
12:28
releasing these new mezzoids into the
12:30
bloodstream.
12:32
This schizogy is what causes the classic
12:35
symptoms of malaria. When millions of
12:38
infected red blood cells rupture
12:40
simultaneously, they release toxins and
12:42
cellular debris into the bloodstream.
12:44
This triggers the immune system and
12:46
causes the characteristic fever, chills,
12:49
and sweating that malaria patients
12:51
experience. The cycle typically repeats
12:54
every 48 hours in plasmodium vivax
12:57
infections, which is why patients often
12:59
experience fever spikes every other day.
13:02
This regular pattern is a hallmark of
13:04
vivax malaria. Not all mezzoids continue
13:07
the cycle of invading new red blood
13:08
cells. Some take a different path
13:11
transforming into special sexual forms
13:13
called gimtoytes. Here we see mezzoids
13:16
that have invaded red blood cells during
13:18
the blood stage of infection. While most
13:20
will continue multiplying asexually,
13:23
some will make a crucial decision.
13:25
Instead of continuing asexual
13:27
reproduction, some mezzoites
13:29
differentiate into gtoytes. This
13:32
differentiation is triggered by specific
13:34
environmental signals and represents the
13:36
parasite preparing for sexual
13:38
reproduction. These gamytes come in two
13:41
distinct forms. Male microgamita shown
13:44
in blue and female macrogita shown in
13:47
pink. The female forms are typically
13:49
larger than the male forms. Male
13:51
microgamita are smaller and will
13:53
eventually produce multiple male
13:55
gameamtes. Female macro gamitoytes are
13:58
larger and contain more cytoplasm
14:00
preparing to become a single female
14:02
gameamt. Let's examine the detailed
14:04
stages of gamty development. This
14:07
diagram shows the various forms that
14:08
parasites take during their development
14:10
in red blood cells.
14:13
This detailed diagram shows how
14:14
plasmodium vivactoytes develop over
14:17
time. Notice the progression from early
14:20
stages to mature male and female forms,
14:23
each with specific proteins that help us
14:25
identify them. The formation of gites is
14:28
crucial because these are the only forms
14:30
that can survive in the mosquito and
14:32
continue the sexual cycle. Without
14:34
gites, the parasite cannot be
14:36
transmitted to new hosts. Gameite
14:39
formation represents a critical decision
14:41
point in the parasite's life cycle. By
14:44
creating these specialized sexual forms,
14:46
plasmodium vivax ensures its survival
14:49
and transmission to new hosts through
14:51
the mosquito vector. The sexual cycle of
14:54
plasmodium vivax begins when a mosquito
14:57
takes a blood meal from an infected
14:59
human. This critical step transfers the
15:02
parasite from one host to another,
15:04
allowing sexual reproduction to occur.
15:06
In the infected human, gimtoytes
15:08
circulate in the bloodstream. These are
15:11
the sexual forms of the parasite ready
15:13
to continue reproduction when they reach
15:15
the mosquito. There are two types of
15:18
gimtoytes. Macrogtoytes which are female
15:21
and microgtoytes which are male. Both
15:24
types must be ingested by the mosquito
15:26
for sexual reproduction to occur. A
15:28
female anophilles mosquito approaches
15:30
the infected human to take a blood meal.
15:33
Only female mosquitoes bite humans as
15:36
they need blood proteins for egg
15:38
development. As the mosquito feeds, it
15:40
sucks up blood containing the gimtoytes.
15:43
This blood meal transfers the sexual
15:45
forms of the parasite from the human
15:47
host into the mosquito's gut.
15:50
Under the microscope, we can see the
15:52
infected red blood cells containing
15:54
gimtotes.
15:55
These parasites are now ready to begin
15:57
sexual reproduction inside the mosquito.
16:01
This ingestion step is crucial in the
16:03
parasites life cycle. It marks the
16:05
transition from the asexual cycle in
16:07
humans to the sexual cycle in
16:09
mosquitoes.
16:11
The ingestion of gimitoytes by the
16:13
mosquito is a critical step that allows
16:15
plasmodium vivax to complete its complex
16:18
life cycle. Without this transfer, the
16:20
parasite cannot reproduce sexually and
16:23
continue its transmission cycle. Inside
16:26
the mosquito's gut, something remarkable
16:28
happens. The gites that were ingested
16:31
during the blood meal are about to
16:32
undergo sexual reproduction. Like the
16:35
parasite having a family reunion inside
16:37
the mosquito. The mosquito's gut
16:40
provides the perfect environment for
16:42
sexual reproduction. Here the male and
16:45
female gtoytes that were ingested with
16:47
the blood meal begin their
16:49
transformation. We have two types of
16:50
gtoytes. The smaller male microtoytes
16:54
and the larger female macrotoytes.
16:57
Both are ready to transform into mature
16:59
gameamtes. The sexual reproduction
17:00
process follows a specific sequence.
17:03
Let's watch as these gito transform into
17:06
gameamtes and undergo fertilization. The
17:08
male gimto underos a process called
17:11
exflagillation.
17:12
It releases multiple threadlike male
17:14
gameamtes each capable of fertilizing a
17:16
female gameamt. Meanwhile, the female
17:19
gito matures into a single large female
17:22
gameamt ready to be fertilized. Now
17:25
comes the magical moment, fertilization.
17:28
One male gameamt approaches and fuses
17:30
with the female gameamt, combining their
17:32
genetic material to form a zygote. The
17:34
result is a zygote, a fertilized cell
17:37
that contains genetic material from both
17:39
parents. This diploid cell is now ready
17:42
for the next stage of development.
17:44
Think of this process as a parasite
17:46
family reunion. The male and female
17:49
parasites meet inside the mosquito,
17:52
combine their genetic recipes, and
17:54
create the next generation that will
17:56
continue the life cycle. This sexual
17:58
reproduction is crucial because it
18:00
creates genetic diversity, helping the
18:02
parasite adapt and survive in different
18:05
environments. The zygote will now
18:07
continue developing into the next stage
18:09
of the life cycle. After fertilization
18:12
in the mosquito's gut, the zygote
18:14
doesn't stay still for long. It underos
18:17
a remarkable transformation into a
18:19
completely different form called an
18:21
ukinite. The zygote transforms into an
18:24
ukinite which is a motile elongated form
18:27
that looks like a tiny worm. This
18:29
transformation gives the parasite the
18:31
ability to move and navigate through the
18:33
mosquito's tissues.
18:35
The ukinite is now equipped with the
18:37
ability to move like a tiny worm. It
18:40
uses this mobility to navigate through
18:42
the mosquito's midgut, which is the
18:44
stomach-like organ where digestion
18:46
occurs.
18:48
The most remarkable part of this process
18:50
is what happens next. The ukinite
18:53
doesn't just float around. It actively
18:55
penetrates the mosquito's midgut wall.
18:58
Think of it like the parasite digging a
19:00
tunnel through the mosquito's stomach
19:01
lining.
19:03
Once the ukinite successfully penetrates
19:06
the midgut wall, it reaches the other
19:08
side where it will undergo its next
19:10
transformation.
19:12
This penetration process is crucial
19:14
because it allows the parasite to escape
19:16
the digestive environment and continue
19:18
its development in a new location within
19:21
the mosquito. The key takeaway is that
19:24
the ukinite represents a critical mobile
19:26
stage that allows the parasite to
19:28
physically move through the mosquito's
19:30
tissues. Without this modile form, the
19:33
parasite couldn't complete its journey
19:34
from the gut to its next developmental
19:37
site.
19:39
Now we enter a crucial multiplication
19:41
phase called sporoggony. Inside the
19:44
protective osis that formed on the
19:45
mosquito's gut wall, the parasite is
19:47
about to build its army through rapid
19:49
asexual reproduction.
19:52
The oasyst starts with a single zygote
19:54
nucleus. This protective cyst attached
19:57
to the mosquito's gut wall provides the
19:59
perfect environment for the parasite to
20:01
multiply safely. This cross-section
20:04
shows the internal structure of a mature
20:06
oyst. You can see the sporocysts
20:09
containing sporosoids, the endroducts of
20:11
sporoggony. Sporoggony begins with the
20:14
zygote nucleus dividing. One becomes two
20:17
through asexual reproduction. This is
20:20
just the beginning of massive
20:21
multiplication. The division continues.
20:24
two becomes four. Each round of division
20:27
doubles the number of nuclei, rapidly
20:29
building up the parasite population.
20:31
After multiple rounds of division, the
20:33
oyst becomes packed with hundreds or
20:35
even thousands of sporosoids.
20:38
This process typically takes 10 to 14
20:41
days depending on temperature. This
20:44
diagram shows the complete sporogy
20:46
process. You can see how the ukinite
20:48
develops into an oicyst and then through
20:51
multiple divisions produces the
20:53
sporosoids that will eventually migrate
20:56
to the mosquito's salivary glands. Think
20:59
of sporoggony as the parasite building
21:01
its army. What starts as a single zygote
21:04
becomes hundreds or thousands of
21:06
sporosoids, each capable of infecting a
21:08
new human host. This massive
21:10
multiplication is what makes malaria
21:12
transmission so efficient. The ocyst
21:15
acts like a factory safely protected on
21:18
the mosquito's gut wall mass-roducing
21:20
the sporosoids that will soon be ready
21:23
for the next phase of transmission back
21:25
to humans. Now we reach the final step
21:28
of the malaria parasites journey through
21:30
the mosquito. The oyst has completed its
21:33
development and is ready to release the
21:35
sporzoids that will infect a new human
21:37
host. Inside the mosquito's gut wall,
21:40
the mature oyst contains thousands of
21:42
sporzoids. These are the infective forms
21:45
of the parasite ready to complete their
21:47
journey. When the oicyst is fully
21:50
mature, it ruptures like a balloon
21:52
bursting releasing thousands of
21:54
sporosoids into the mosquito's body
21:56
cavity.
21:58
The released sporzoids don't stay in the
22:00
body cavity. They have a specific
22:02
destination, the mosquito's salivary
22:04
glands located near the head. Watch as
22:07
the sporzoites migrate through the
22:09
mosquito's body following chemical
22:11
signals that guide them to the salivary
22:13
glands. This journey takes about 10 to
22:17
14 days after the mosquito's initial
22:19
blood meal.
22:21
Now the mosquito is ready to transmit
22:23
malaria. When it takes its next blood
22:26
meal from a human, it will inject saliva
22:28
containing sporzoids directly into the
22:31
person's bloodstream. The sporzoids are
22:33
now perfectly positioned in the salivary
22:35
glands. As the mosquito feeds, it
22:38
injects these parasites along with
22:39
anti-coagulants to keep the blood
22:41
flowing. This completes the transmission
22:44
back to humans. And so the malaria life
22:46
cycle comes full circle from human to
22:49
mosquito and back to human again. Each
22:52
infected mosquito can potentially infect
22:54
multiple people during its lifetime,
22:56
which is why malaria spreads so
22:58
effectively in endemic areas.
23:01
Now we reach the heart of why plasmodium
23:03
vivax is such a challenging parasite to
23:06
eliminate. The hypnosits we learned
23:08
about earlier create a major problem for
23:11
treatment and control efforts.
23:14
Here we can see how hypnosits create a
23:16
persistent infection. These dormant
23:18
forms hide in liver cells completely
23:21
undetectable by our current diagnostic
23:23
methods. They can remain silent for
23:26
weeks, months, or even years before
23:28
suddenly reactivating.
23:30
Let me show you the typical pattern of
23:32
vivax malaria relapses. A patient gets
23:35
infected, receives treatment, and
23:37
appears to be cured, but then weeks or
23:39
months later, the symptoms return as
23:41
hypnosits reactivate and cause new blood
23:44
infections.
23:45
This diagram shows why standard malaria
23:48
treatment often fails with vivax
23:50
malaria. Most antimmalarial drugs only
23:53
kill the parasites circulating in the
23:55
blood. They cannot reach the dormant
23:57
hypnosits hiding in liver cells which
23:59
means the source of future relapses
24:01
remains untouched.
24:04
The key takeaway is that treating vivac
24:06
malaria requires what we call radical
24:08
cure. This means using medications that
24:11
target both the blood stages causing
24:13
current symptoms and the liver hypnosits
24:16
that cause future relapses.
24:18
Only by eliminating both can we truly
24:21
cure the infection and prevent the cycle
24:23
of relapses that makes vivax malaria so
24:26
persistent. A radical cure means
24:28
completely eliminating the parasite from
24:30
your body, including those sneaky
24:31
hypnosits hiding in the liver. Unlike
24:34
regular treatment that only targets
24:36
parasites in the blood, radical cure
24:39
goes after the dormant forms, too.
24:41
Without radical cure, these hypnosits
24:44
can reactivate weeks, months, or even
24:46
years later, causing relapse infections.
24:49
This is why some people get malaria
24:51
again even after successful treatment of
24:53
their blood infection.
24:56
Two main drugs can achieve radical cure,
24:58
primacquine and tephen. These
25:00
medications specifically target the
25:02
hypnosits in the liver, ensuring
25:04
complete elimination of the parasite.
25:06
Watch as these drugs target and
25:08
eliminate the hypnosits. The medication
25:11
travels to the liver and specifically
25:13
attacks these dormant parasites,
25:15
preventing future relapses.
25:18
However, there's a crucial safety
25:20
requirement before using these drugs.
25:22
Patients must be tested for G6PD
25:24
deficiency, a genetic condition that
25:27
affects red blood cells. People with
25:29
G6PD deficiency can experience dangerous
25:32
side effects from these medications,
25:34
including severe anemia. That's why
25:36
testing is mandatory before starting
25:38
radical cure treatment.
25:40
This diagram shows how different drugs
25:42
target different stages of the parasite
25:44
life cycle. Artemisin targets the blood
25:47
stage while primacqueen specifically
25:50
targets the hypnosid stage in the liver
25:52
achieving true radical cure. Radical
25:55
cure is essential for truly defeating
25:57
pivax malaria. By eliminating both
25:59
bloodstage parasites and liver
26:01
hypnosits, we can prevent relapses and
26:04
break the cycle of infection. But
26:06
remember, G6 PD testing comes first for
26:09
patient safety. Before patients can
26:11
safely receive Primacqueen or
26:12
Tofphenqueen for radical cure of Pivvax
26:15
malaria, there's a critical safety step
26:17
that must never be skipped. Testing for
26:20
G6PD deficiency. Both Primocqueen and
26:23
Tephenocqueen are essential medications
26:25
for eliminating the dormant hypnosits in
26:28
the liver. However, these drugs can
26:30
cause severe complications in people
26:32
with G6PD deficiency. G6PD deficiency is
26:36
the most common enzyme deficiency
26:37
worldwide, affecting over 400 million
26:40
people. G6PD stands for glucose 6
26:43
phosphate dehydrogenase, an enzyme that
26:46
protects red blood cells from oxidative
26:48
damage. This biochemical pathway shows
26:50
how G6PD works. The enzyme converts
26:53
glucose 6 phosphate and produces NADPH,
26:56
a crucial molecule that acts like a
26:58
cellular antioxidant, protecting red
27:00
blood cells from damage caused by
27:01
oxidative stress.
27:03
When someone has G6PD deficiency, their
27:06
red blood cells cannot produce enough
27:08
NADPH to protect themselves. If they
27:11
take primocqueen or taffen, the
27:13
oxidative stress can cause severe
27:15
hemolytic anemia. Under the microscope,
27:17
we can see the devastating effects. The
27:20
damaged red blood cells form
27:21
characteristic shapes called bite cells
27:24
and blister cells, which are clear signs
27:25
of hemolytic anemia caused by G6PD
27:28
deficiency.
27:30
This is why G6PD testing is absolutely
27:33
essential before starting radical cure
27:35
treatment. The test is simple, quick,
27:38
and can prevent life-threatening
27:39
complications. Remember, G6PD testing
27:42
isn't just a recommendation. It's a
27:45
life-saving requirement. No patient
27:47
should receive Primocqueen or
27:48
Tephenocqueen without first confirming
27:50
their G6PD status. This simple test
27:53
makes the difference between safe,
27:55
effective treatment and potentially
27:57
fatal complications. Drug resistance in
28:00
plasmodium vivax is becoming an
28:02
increasingly serious problem worldwide.
28:04
What was once easily treatable with
28:06
standard medications is now requiring
28:08
new approaches and constant vigilance.
28:11
Drug resistance occurs when parasites
28:13
develop genetic mutations that allow
28:15
them to survive despite treatment with
28:17
antimmalarial drugs. This leads to
28:20
treatment failures and makes infections
28:22
much harder to cure.
28:25
Chloricquin has been the go-to treatment
28:27
for pivox malaria for decades. It works
28:30
by preventing parasites from detoxifying
28:33
heem, a toxic byproduct of digesting
28:35
hemoglobin. When he accumulates, it
28:37
kills the parasite.
28:40
Resistance develops through natural
28:42
selection. Random genetic mutations
28:44
occasionally allow some parasites to
28:46
survive chlorocqueen treatment. These
28:49
resistant parasites then multiply and
28:51
spread, leading to increasing treatment
28:53
failures. in affected areas.
28:56
Chloricquin resistance in pivox has been
28:59
documented in several regions worldwide.
29:02
Southeast Asia, particularly Papa New
29:04
Guinea and Indonesia, shows the highest
29:06
levels of resistance. Parts of South
29:09
America and Oceanania are also reporting
29:11
treatment failures.
29:14
When chloricquin fails, doctors turn to
29:16
armin based combination therapies or
29:19
ACTs. These combine are artemine
29:21
derivatives with other antimmalarial
29:23
drugs. Common combinations include
29:26
artamethylumantrine and artisunate
29:28
mephloquin which are more effective
29:30
against resistant parasites.
29:33
Continuous monitoring of drug resistance
29:35
is essential for effective malaria
29:37
control. It helps track the spread of
29:40
resistant parasites, allows for rapid
29:42
updates to treatment guidelines, and
29:44
guides public health interventions to
29:46
prevent widespread treatment failures.
29:50
Drug resistance in Pivax represents a
29:53
significant challenge to malaria control
29:55
efforts. While chlorocqueen resistance
29:57
is spreading, effective alternatives
29:59
like ACTs are available. The key is
30:02
maintaining robust surveillance systems
30:05
to detect resistance early and adapt
30:07
treatment strategies accordingly.
30:12
Countries around the world are
30:14
implementing comprehensive strategies to
30:16
eliminate plasmodium vivax malaria.
30:19
This global effort requires multiple
30:21
approaches working together to break the
30:24
transmission cycle. PVA is most common
30:27
in tropical regions outside Africa
30:29
particularly in Asia Pacific and South
30:31
America. Unlike Palsiparam, vivac can
30:34
survive in cooler temperatures making it
30:36
geographically widespread.
30:39
Elimination efforts focus on four main
30:41
strategies that work together to
30:43
interrupt transmission and prevent
30:45
relapses. First, improved case
30:48
management ensures patients receive
30:49
early diagnosis, appropriate treatment,
30:52
including radical cure, and proper
30:54
followup to prevent relapses. Second,
30:57
vector control targets anophles
30:59
mosquitoes through bed nets, indoor
31:01
residual spraying, and eliminating
31:03
breeding sites to reduce transmission.
31:06
Third, mass drug administration treats
31:08
entire populations to clear both active
31:10
infections and dormant hypnosits,
31:13
breaking the transmission cycle. Fourth,
31:16
regional collaboration coordinates
31:17
efforts across borders as infected
31:19
people can easily travel between
31:21
countries, requiring shared strategies
31:24
and data.
31:26
These prevention methods work together
31:28
as part of comprehensive elimination
31:30
programs. Each method targets different
31:33
aspects of transmission from protecting
31:36
individuals to reducing mosquito
31:38
populations.
31:40
Mass drug administration is a powerful
31:42
tool that treats entire communities, not
31:45
just diagnosed cases. This approach
31:48
targets the hidden reservoir of
31:49
infections and dormant hypnosits that
31:52
maintain transmission.
31:54
Several countries are leading
31:55
elimination efforts. Thailand has proven
31:58
that G6PD testing and tophenqueen
32:01
treatment are operationally feasible.
32:03
Brazil became the first country to
32:05
implement nationwide tophenqueen
32:07
programs. Pakistan is developing
32:10
comprehensive elimination roadmaps.
32:12
Despite progress, significant challenges
32:14
remain. Crossber movement can
32:17
reintroduce infections. Remote areas
32:19
have limited access to proper treatment
32:21
and maintaining long-term programs
32:23
requires sustained commitment and
32:25
resources.
32:27
The fight against Pivax requires
32:29
coordinated global efforts combining
32:31
improved health care, vector control,
32:34
mass treatment programs, and
32:36
international cooperation. While
32:38
challenges exist, countries are proving
32:40
that elimination is achievable with
32:42
sustained commitment and proper
32:44
resources.
32:46
New breakthrough drugs are
32:48
revolutionizing the fight against
32:50
plasmodium vivax malaria.
32:52
The most significant advancement is
32:54
Tephenoqueen, a game-changing medication
32:57
that offers hope for better treatment
32:59
outcomes. Tofenqueen is a revolutionary
33:01
antimmalarial drug that specifically
33:03
targets the dormant hypnosits in the
33:06
liver. Unlike older treatments, it can
33:08
be given as a single dose and
33:10
effectively prevents the relapses that
33:12
make Pivax so challenging to treat.
33:16
In 2023, Brazil made history by becoming
33:19
the first country in the world to
33:21
incorporate Tephenocqueen and
33:23
quantitative G6PD testing into their
33:26
national malaria treatment program. This
33:28
groundbreaking implementation covers
33:30
patients 16 years and older across the
33:33
entire country.
33:35
Thailand has conducted crucial
33:37
feasibility studies showing that point
33:39
of care G6PD testing combined with
33:42
tphenocquin treatment is operationally
33:45
feasible within their public health
33:46
service. This research proves that the
33:49
new approach can work in real world
33:51
health care settings.
33:54
G6PD testing is absolutely critical
33:56
because tphenocqueen can cause dangerous
33:59
hemolytic anemia in people with G6PD
34:01
deficiency. The development of point of
34:03
care quantitative G6PD tests has made it
34:06
possible to safely prescribe tphenocquin
34:08
by identifying at risk patients before
34:11
treatment.
34:13
This progress represents a major
34:14
breakthrough in pivax treatment. The
34:17
combination of single dose to phenqueen
34:19
with reliable G6PD testing transforms
34:22
patient care from complex multid-dosese
34:25
regimens with poor compliance to simple,
34:27
safe and effective treatment that
34:29
actually prevents relapses. The
34:31
implementation of Tephenocqueen with
34:33
quantitative G6PD testing represents one
34:36
of the most significant advances in
34:38
malaria treatment in decades.
34:41
Countries like Brazil and Thailand are
34:43
leading the way, showing that this new
34:45
approach can work in real world health
34:47
care systems and dramatically improve
34:49
outcomes for Pivax patients. The fight
34:52
against plasmodium vivax malaria is
34:55
entering an exciting new phase.
34:57
Researchers worldwide are developing
34:59
innovative tools and strategies to
35:01
overcome the unique challenges this
35:03
parasite presents.
35:05
Before we look at solutions, let's recap
35:07
the main challenges. Hypnosoits remain
35:10
hidden in liver cells. Drug resistance
35:12
is spreading. Current detection methods
35:14
have limitations and testing for G6PD
35:17
deficiency is complex.
35:20
Scientists are developing next
35:22
generation antimmalarial drugs
35:23
specifically designed to target dormant
35:26
hypnosits in liver cells. These new
35:28
compounds aim to overcome existing drug
35:31
resistance while being safer for
35:32
patients with G6PD deficiency.
35:36
Diagnostic tools are becoming more
35:38
sophisticated and accessible. New rapid
35:41
diagnostic tests can quickly detect
35:43
peavvax infections in the field, helping
35:46
healthare workers distinguish between
35:48
different malaria species and start
35:50
appropriate treatment faster.
35:53
The future of malaria diagnostics
35:55
involves a multi-level approach from
35:57
high throughput testing at national
35:59
reference levels to simple rapid tests
36:02
at the community level. This strategy
36:04
ensures appropriate diagnostic tools are
36:06
available at every healthcare setting.
36:10
Point of care G6PD testing is
36:12
revolutionizing treatment decisions.
36:14
These portable devices provide
36:16
quantitative results in minutes,
36:19
allowing healthare workers to safely
36:21
prescribe radical cure treatments even
36:23
in remote areas where laboratory testing
36:26
isn't available.
36:27
These advances work together as an
36:29
integrated strategy. New drugs that
36:32
target hypnosits combined with better
36:34
diagnostic tools and point of care G6PD
36:36
testing create a powerful toolkit for
36:39
eliminating pivax malaria from affected
36:41
regions. The future looks promising.
36:44
With these new tools and strategies,
36:46
researchers and healthcare workers are
36:48
getting closer to achieving the ultimate
36:50
goal, a world free of P vivvax malaria.
36:54
We've journeyed through the intricate
36:55
world of plasmodium vivac exploring
36:58
every stage of its complex life cycle.
37:01
While this parasite presents significant
37:03
challenges, it's important to remember
37:05
that knowledge is our greatest weapon in
37:07
this fight.
37:09
The life cycle of pivox involves
37:12
multiple stages across two different
37:13
hosts, humans and mosquitoes. From
37:16
sporzoites to hypnosites, from
37:18
mezazoites to gito, each stage presents
37:21
both challenges and opportunities for
37:23
intervention.
37:25
But here's the encouraging news. We have
37:27
powerful tools at our disposal.
37:30
Prevention through vector control and
37:32
bed nets, effective treatment with
37:34
radical cure approaches like tphenoquin,
37:36
and coordinated elimination efforts
37:38
worldwide are all making a real
37:41
difference.
37:42
Our detailed understanding of each
37:45
parasite stage from the ring forms in
37:47
blood cells to the complex gtoytes gives
37:50
us the knowledge we need to target
37:52
vulnerable points, develop better
37:54
diagnostics, create new treatments, and
37:57
prevent transmission.
37:59
Real progress is happening around the
38:01
world. Brazil became the first country
38:03
to implement Taffenquin nationwide.
38:06
Thailand successfully integrated G6PD
38:08
testing. The Mikong region saw a 27%
38:11
decrease in malaria cases. These
38:13
successes prove that Pivax is indeed
38:16
conquerable.
38:18
Plasmodium vivax may be complex, but it
38:21
is absolutely conquerable through
38:23
continued research, global cooperation,
38:25
and the dedication of healthare workers
38:27
worldwide. We are making real progress.
38:29
Stay informed, stay protected, and
38:31
remember, every person who understands
38:34
this parasite becomes part of the
38:35
solution. Together we can and will end
38:39
malaria.
#Public Health