Up next in 10

Lymphatic Filariasis: Unraveling the Wuchereria bancrofti Parasite
Website: https://biologynotesonline.com/
Facebook: https://www.facebook.com/biologynotesonline
Instagram: https://www.instagram.com/biologynotesonline/?hl=en
Show More Show Less View Video Transcript
0:00
Hey everyone, today we're diving into
0:02
the world of Wukaria Bankraftoft, a tiny
0:05
but mighty parasite that affects
0:07
millions of people worldwide. Let's
0:09
start with the basics. Wukaria Bankrofty
0:12
is a nematode, which is a fancy
0:14
scientific term for roundorm. But don't
0:16
let it simple name fool you. This
0:18
microscopic creature is incredibly
0:20
complex.
0:22
Here's what
0:24
actually looks like under a microscope.
0:26
This purple stained specimen shows the
0:28
characteristic long slender body that's
0:31
coiled in a distinctive shape.
0:34
This tiny parasite is the main culprit
0:37
behind a disease called lymphatic
0:38
ferasis. It's responsible for about 90%
0:42
of all cases worldwide. This world map
0:45
shows just how widespread this problem
0:47
is. The colored regions represent
0:50
countries where lymphatic ferasis is
0:52
endemic with Africa, parts of Asia, and
0:55
some areas of South America being most
0:57
affected.
0:58
Now, here's a helpful way to think about
1:00
what this parasite does. Imagine your
1:04
body has a sophisticated drainage
1:06
system. That's your lymphatic system. It
1:08
helps remove excess fluid and waste from
1:10
your tissues.
1:12
Wukaria bankrofty is like a microscopic
1:15
intruder that invades this drainage
1:17
system. It sets up camp in your
1:19
lymphatic vessels and nodes causing
1:22
blockages and inflammation that can lead
1:24
to serious health problems.
1:27
So remember wukaria bankrofti may be
1:29
tiny but its impact is enormous. This
1:33
roundworm parasite is the leading cause
1:35
of lymphatic feriosis affecting millions
1:37
of people by disrupting one of our
1:39
body's most important systems.
1:42
Now let's take a closer look at the worm
1:44
itself. Understanding the physical
1:46
characteristics of wukaria bankrofty
1:48
helps us recognize how this parasite
1:50
adapts to life inside the human body.
1:54
Adult wukaria bankrofty worms have a
1:56
distinctive threadlike appearance.
1:59
They're quite long for parasites
2:01
measuring several centimeters in length
2:03
and they make their home in the human
2:05
lymphatic system specifically in the
2:07
lymph nodes. To put this in perspective,
2:10
adult worms can range from 4 to 10 cm in
2:13
length. The females are typically larger
2:16
than the males, which is common in many
2:18
parasitic species.
2:20
The female worms produce tiny offspring
2:23
called microfilaria.
2:25
These microscopic larae are released
2:27
directly into the bloodstream where they
2:29
circulate throughout the body. Here we
2:32
can see a detailed diagram of a
2:33
microfilaria.
2:35
Notice the internal structures that are
2:37
visible through its translucent body,
2:40
including the nerve ring and other
2:41
cellular components. This microscopic
2:44
view shows actual microfilaria in blood
2:47
samples. You can see the characteristic
2:49
wormlike shape and how they appear among
2:51
the blood cells. Some have distinctive
2:54
features like blunt tails that help in
2:56
identification.
2:58
To understand the dramatic size
3:00
difference, adult worms measure several
3:02
centimeters, while microfilaria are only
3:05
about 0.2 to 0.3 mm long. That's roughly
3:09
twice the width of a human hair. The key
3:12
characteristics to remember are that
3:14
adult worms are thread-like parasites
3:16
living in lymph nodes, while
3:17
microfilaria are their microscopic
3:19
offspring circulating in the
3:21
bloodstream. This two-stage existence is
3:23
crucial for the parasite survival and
3:26
transmission cycle.
3:28
Understanding the life cycle of wukaria
3:30
bankrofti is essential to grasp how this
3:33
parasite spreads between humans and
3:35
causes lymphatic valeriosis. This
3:37
complex cycle involves two hosts,
3:40
mosquitoes and humans. Here we see the
3:42
complete life cycle diagram. Notice how
3:45
the cycle alternates between the
3:46
mosquito vector and the human host with
3:49
specific developmental stages occurring
3:51
in each.
3:53
The cycle begins when a female mosquito
3:55
bites an infected person. During blood
3:58
feeding, the mosquito ingests tiny
4:00
wormlike creatures called microfaria
4:03
that circulate in the infected person's
4:05
bloodstream. Inside the mosquito, these
4:07
microfaria don't remain dormant. Over
4:10
the next 10 to 14 days, they undergo
4:13
development, molting twice to become
4:15
infective third stage larvae known as L3
4:18
larvae. These mature L3 larae then
4:21
migrate through the mosquito's body to
4:23
reach the probosus, the needle-like
4:25
mouth part used for blood feeding. Now
4:28
the mosquito is ready to transmit the
4:30
infection.
4:32
When this infected mosquito bites
4:34
another person, the L3 larae are
4:36
deposited onto the skin surface near the
4:38
bite wound. These microscopic larvae
4:41
then actively enter the human body
4:44
through the mosquito bite. Once inside
4:46
the human host, the larae begin an
4:48
incredible journey. They migrate through
4:50
tissues to reach the lymphatic system,
4:53
the body's network of vessels that help
4:55
fight infection and maintain fluid
4:57
balance. In the lymphatic vessels, the
4:59
larve undergo further development over 6
5:02
to 8 months, growing into adult worms.
5:05
These adult worms can live for 4 to 6
5:07
years in the human lymphatic system.
5:11
Here's another view of the complete
5:13
cycle. The adult worms in the lymphatic
5:15
system mate and produce millions of
5:18
microfilaria
5:19
which circulate in the bloodstream ready
5:22
to be picked up by the next mosquito
5:23
bite. This completes the cycle. The
5:26
microfilaria in the blood are now
5:28
available for uptake by mosquitoes
5:30
perpetuating the transmission cycle and
5:33
spreading the infection to new hosts.
5:36
Understanding this life cycle reveals
5:38
why controlling lymphatic feriosis
5:41
requires targeting both the mosquito
5:42
vector and treating infected humans.
5:46
Breaking any part of this cycle can stop
5:48
transmission and prevent new infections.
5:51
Mukaria bankrofty has a specific
5:53
geographic distribution pattern that
5:55
tells us a lot about the conditions it
5:57
needs to survive and spread.
6:00
This parasite is primarily found in
6:02
tropical and subtropical regions around
6:05
the world. Let's look at a global
6:07
distribution map to see exactly where
6:09
it's most prevalent. The red areas on
6:12
this map show where wooaria bankrofti is
6:15
endemic. Notice how it's concentrated in
6:17
specific regions of Africa, Asia, South
6:19
America, and the Pacific Islands. Here's
6:22
another view showing the endemic
6:24
countries and territories more clearly.
6:27
This map helps us understand the global
6:29
scope of lymphatic valeriosis. The major
6:32
endemic regions include subsaharan
6:34
Africa, South and Southeast Asia,
6:37
Pacific Islands, and parts of South
6:39
America. Each of these regions has
6:41
specific environmental conditions that
6:43
favor transmission. The numbers are
6:46
staggering. Over 120 million people are
6:49
currently infected with Wukaria
6:51
Bankrofty worldwide and nearly 900
6:54
million people are at risk of infection.
6:58
Several key factors contribute to the
7:00
spread of weria bankrofty. Poor
7:02
sanitation creates breeding grounds for
7:04
mosquitoes while inadequate vector
7:07
control allows mosquito populations to
7:09
thrive. Tropical and subtropical
7:11
climates provide the warm, humid
7:13
conditions that both mosquitoes and the
7:16
parasite need to survive. Additionally,
7:19
poverty limits access to health care and
7:21
prevention measures. The key takeaway is
7:24
that Wueria Bankraftoft thrives in
7:27
tropical regions where poor sanitation,
7:29
inadequate mosquito control, and poverty
7:31
create ideal conditions for
7:33
transmission. Understanding this
7:35
distribution helps guide prevention and
7:37
control efforts.
7:39
Mosquitoes are the unsung carriers in
7:41
the story of lymphatic feriosis. These
7:44
tiny insects serve as vectors
7:46
transporting wukaria bankrofty from
7:48
person to person without us even
7:49
realizing it. Four main mosquito genera
7:52
can transmit wukuraria bankrofty. Each
7:56
has different characteristics and
7:57
preferred habitats but all can carry
7:59
this dangerous parasite. Understanding
8:01
the mosquito life cycle is crucial for
8:04
control efforts. Here we see how
8:06
anophles mosquitoes develop from eggs
8:08
laid on water surfaces through laral and
8:11
pupil stages to become adult disease
8:13
vectors. Mosquito larve develop in
8:16
standing water hanging upside down from
8:18
the surface to breathe. These aquatic
8:21
breeding sites are critical points for
8:23
mosquito control interventions.
8:25
Aquatic plants like water hyasin create
8:28
perfect mosquito breeding habitats.
8:30
These plants provide shelter and
8:32
nutrients, making water bodies ideal
8:34
nurseries for mosquito larve. The
8:37
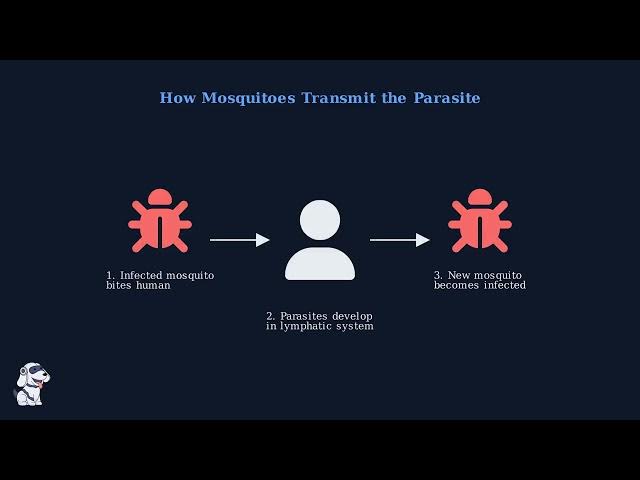
transmission process is straightforward
8:39
but deadly effective. An infected
8:41
mosquito bites a human, depositing
8:44
parasite larve. These larve mature in
8:46
the lymphatic system and when another
8:48
mosquito bites the infected person, it
8:50
picks up microfilaria to continue the
8:52
cycle. Controlling mosquito populations
8:55
is essential for preventing lymphatic
8:57
feriosis. This involves eliminating
9:00
breeding sites, using insecticides, and
9:03
implementing community-based prevention
9:05
programs. Remember, mosquitoes are not
9:08
just annoying pests. They are dangerous
9:10
disease vectors. Understanding their
9:13
role in transmitting wukaria bankrofty
9:15
helps us develop better strategies to
9:17
protect communities from lymphatic
9:19
feriosis. Understanding how wukaria
9:22
bankrofty makes us sick requires looking
9:24
at what happens when adult worms take up
9:27
residence in our lymphatic system. The
9:29
pathogenesis involves both direct damage
9:32
from the worms and our body's immune
9:34
response. First, let's understand the
9:37
normal lymphatic system. This network of
9:40
vessels and nodes drains excess fluid
9:42
from our tissues and returns it to the
9:44
bloodstream, maintaining proper fluid
9:46
balance throughout our body. When adult
9:49
wukaria bankroftey worms establish
9:52
themselves in the lymphatic vessels,
9:54
they physically block the normal flow of
9:56
lymphatic fluid. These worms can live
9:59
for years creating chronic obstruction
10:01
in the lymphatic system. The disease
10:04
progresses in stages. Initially blocked
10:06
lymphatic drainage causes fluid to
10:08
accumulate in tissues leading to
10:10
swelling called lympadema. The affected
10:13
limb becomes enlarged as fluid builds up
10:15
in the tissue spaces.
10:18
In severe cases, the condition
10:20
progresses to elephantiasis.
10:22
The affected limb becomes massively
10:24
swollen with thickened hardened skin.
10:26
This represents the end stage of the
10:28
disease, causing permanent disfigurement
10:30
and significant disability.
10:33
The body's immune system recognizes the
10:35
worms as foreign invaders and mounts an
10:38
inflammatory response. However, this
10:41
chronic inflammation actually
10:42
contributes to the tissue damage. The
10:45
immune response causes scarring and
10:47
further blocks lymphatic flow, worsening
10:49
the condition.
10:51
To summarize the pathogenesis,
10:54
adult worms physically block lymphatic
10:56
drainage, leading to fluid accumulation
10:59
and progressive swelling. The body's
11:01
immune response while trying to fight
11:03
the infection actually worsens the
11:05
tissue damage through chronic
11:07
inflammation, ultimately causing the
11:09
permanent changes we see in lymphatic
11:11
ferasis.
11:15
Wukaria bankrofty infections can present
11:17
in three distinct ways ranging from
11:20
completely silent infections to severe
11:22
lifealtering symptoms. Understanding
11:25
these manifestations is crucial for
11:27
recognizing and treating lymphatic
11:29
valeriosis.
11:31
Most infections are actually
11:32
asymptomatic, meaning people show no
11:35
visible symptoms but still suffer
11:37
internal lymphatic damage. Acute
11:39
symptoms appear during active
11:41
inflammation while chronic symptoms
11:43
represent permanent damage from
11:45
long-term infection.
11:48
The most concerning aspect of lymphatic
11:50
feriosis is that most people don't even
11:52
know they're infected. Between 70 and
11:55
80% of infections are completely
11:57
asymptomatic.
11:59
Yet, the parasites are still causing
12:01
damage to the lymphatic system and
12:03
kidneys.
12:05
Acute symptoms occur when the immune
12:07
system actively fights the parasites.
12:09
Patients experience high fever, swollen
12:12
and painful lymph nodes, and red streaks
12:15
along the skin following lymphatic
12:17
vessels. These episodes can last several
12:19
days and often lead to secondary
12:21
bacterial infections.
12:24
Chronic lympadeema is the most visible
12:26
sign of long-term infection. When adult
12:28
worms block lymphatic vessels, fluid
12:31
accumulates in tissues causing permanent
12:33
swelling. This typically affects the
12:35
legs but can also involve arms and other
12:38
body parts. In severe cases, lympadeema
12:42
progresses to elephantis where limbs
12:45
become massively enlarged with thick
12:47
hardened skin resembling elephant hide.
12:50
This devastating condition severely
12:51
impacts mobility and quality of life
12:54
making simple daily activities extremely
12:56
difficult. Hydrail is a malespecific
13:00
manifestation where fluid accumulates
13:02
around the testicles causing scrotal
13:04
swelling and discomfort. This affects up
13:07
to 40% of infected men and can be
13:10
surgically treated though it may recur
13:12
if the underlying infection isn't
13:14
eliminated.
13:16
The key clinical insight is that
13:18
lymphatic ferasis often progresses
13:20
silently from asymptomatic infection to
13:23
irreversible chronic manifestations.
13:26
Early detection and treatment are
13:27
crucial to prevent permanent disability,
13:30
though even established chronic symptoms
13:32
can be managed to improve quality of
13:34
life. Diagnosing lymphatic valeriosis
13:37
requires finding evidence of wukaria
13:40
bankrofi in the patient's body. This
13:42
presents unique challenges because the
13:44
parasites have specific behaviors and
13:46
locations that affect when and how we
13:49
can detect them. The first method
13:51
involves analyzing blood samples under a
13:53
microscope to find microfilaria, the
13:56
laral stage of the worm. However, timing
13:59
is crucial because these parasites show
14:01
nocturnal periodicity, meaning they're
14:03
most active in the bloodstream at night.
14:07
During the day, microfilaria hide in the
14:09
lungs and deeper blood vessels, making
14:11
them difficult to detect. At night,
14:14
typically between 10 p.m. and 2 a.m.,
14:17
they migrate to peripheral blood vessels
14:19
where they can be easily found in blood
14:20
samples.
14:23
Under the microscope, we can see the
14:25
characteristic C-shaped microfilar. They
14:28
appear as purple stained translucent
14:30
worms with visible internal structures.
14:33
This microscopic examination remains the
14:35
gold standard for confirming active
14:37
infection.
14:39
Circulating ferial antigen tests
14:42
represent a major breakthrough in
14:43
diagnosis. Unlike traditional blood
14:46
microscopy that requires nighttime
14:48
collection, CFA tests can be performed
14:50
any time of day and provide quick,
14:53
highly sensitive results. CFA tests
14:56
detect proteins released by adult worms
14:58
living in the lymphatic system. These
15:01
antigens circulate constantly in the
15:03
blood making timing irrelevant. The
15:05
tests are so sensitive they can detect
15:07
infections even when no microfilaria are
15:10
visible under the microscope.
15:13
Additional diagnostic methods include
15:15
molecular tests using PCR to detect
15:17
parasite DNA, antibbody tests that
15:20
measure the body's immune response, and
15:22
ultrasound imaging that can sometimes
15:24
visualize adult worms moving in
15:26
lymphatic vessels, a phenomenon called
15:28
the farial dance sign.
15:31
The key takeaways for diagnosing
15:33
lymphatic feriosis are timing is
15:36
critical for traditional blood tests.
15:38
CFA tests have revolutionized diagnosis
15:40
with their convenience and sensitivity.
15:43
Using multiple diagnostic methods
15:45
improves accuracy and early detection is
15:48
essential for effective treatment and
15:50
preventing long-term complications. When
15:52
someone is infected with wooaria
15:54
bankrofti, we have several effective
15:57
medications to fight this parasitic
15:59
infection. The key is using the right
16:01
combination of drugs to eliminate both
16:03
the adult worms and the circulating
16:06
microfaria.
16:07
Dithylcarbamazine or D is our primary
16:10
weapon against lymphatic feriosis. This
16:13
medication is unique because it can kill
16:15
both the adult worms living in the
16:17
lymphatic system and the microfilaria
16:20
circulating in the blood. However,
16:22
modern treatment often uses combination
16:24
therapy. By combining DEC with other
16:27
medications like alendazol or
16:29
ivormectin, we can achieve better
16:31
results and reduce the chance of
16:33
treatment failure. Doxycycline
16:35
represents an exciting development in
16:37
treatment. Unlike other medications that
16:39
directly target the worm, doxycycline
16:42
works by targeting wbakia bacteria that
16:44
live inside the worms and it has
16:46
powerful anti-inflammatory effects.
16:49
Treatment isn't just about giving
16:51
medications. We must carefully consider
16:53
side effects, patient safety, and
16:56
special situations.
16:58
For example, in areas where loasis is
17:00
common, we avoid D because it can cause
17:02
dangerous reactions. Successful
17:04
treatment requires a comprehensive
17:06
approach. We don't just give pills and
17:09
walk away. Patients need ongoing care to
17:12
manage symptoms, prevent complications,
17:14
and ensure the infection is completely
17:16
eliminated. The key to successful
17:18
treatment is using the right combination
17:20
of medications, monitoring patients
17:23
carefully, and providing comprehensive
17:25
care that addresses both the infection
17:28
and its complications.
17:30
With proper treatment, we can eliminate
17:32
the worms and help patients recover
17:34
their health. In the year 2000, the
17:37
World Health Organization launched an
17:38
ambitious global initiative that would
17:41
change the fight against lymphatic
17:42
ferasis forever. This program is called
17:45
the global program to eliminate
17:47
lymphatic feriosis or GPLF. The primary
17:51
goal of GPLF is straightforward yet
17:53
ambitious to eliminate lymphatic
17:56
falariosis as a public health problem
17:58
worldwide. This means reducing the
18:01
disease to such low levels that it no
18:03
longer poses a significant threat to
18:05
communities. GPL operates on a
18:07
two-pillar strategy. The first pillar
18:09
focuses on interrupting transmission
18:12
through mass drug administration while
18:14
the second pillar manages morbidity and
18:17
prevents disability in those already
18:19
affected. Mass drug administration
18:21
involves giving preventive medications
18:23
to entire atrisisk populations typically
18:26
once a year. This approach treats
18:28
infected individuals and prevents new
18:31
infections gradually breaking the cycle
18:33
of transmission in communities. The
18:35
second pillar focuses on helping people
18:37
who already have chronic symptoms of
18:39
lymphatic valerosis. This includes
18:41
managing lympadeema, treating secondary
18:44
infections, and providing care to
18:46
improve quality of life and prevent
18:48
further disability.
18:50
Together, these two pillars work to both
18:53
interrupt transmission and alleviate the
18:55
suffering of those affected. GPELF
18:58
represents a comprehensive approach that
19:00
addresses both prevention and care,
19:03
making it one of the most successful
19:05
global health initiatives in modern
19:07
history. The global program to eliminate
19:09
lymphatic feriosis has achieved
19:12
remarkable progress since its launch in
19:14
2000, but significant challenges remain
19:17
on the path to complete elimination.
19:20
Since the program began, there has been
19:22
a dramatic 74% decline in lymphatic
19:25
ferasis infections worldwide.
19:28
This represents one of the most
19:29
successful global health initiatives in
19:32
recent history. The scale of this effort
19:34
is unprecedented. Over 9.7 billion
19:37
cumulative treatments have been
19:38
delivered to atrisisk populations and
19:41
871 million people no longer require
19:44
preventive chemotherapy. This success is
19:46
the result of unprecedented global
19:48
collaboration.
19:50
The global program brings together
19:52
ministries of health, donors,
19:54
pharmaceutical companies, academic
19:55
institutions, and NOS's working toward a
19:58
common goal. However, despite this
20:00
remarkable progress, significant
20:02
challenges continue to impede complete
20:04
elimination of lymphatic feriosis
20:07
worldwide. The first major challenge is
20:09
loasis co-endemicity. In areas where
20:12
both lymphatic ferasis and loasis occur
20:15
together, standard treatments like DC
20:17
and ivormectin can cause severe adverse
20:20
reactions in patients with high loasis
20:22
infection levels. The second critical
20:24
challenge is achieving complete
20:26
geographic coverage with mass drug
20:28
administration. Many programs struggle
20:31
to reach 100% of target populations due
20:34
to accessibility barriers, compliance
20:36
issues, and resource constraints. These
20:39
challenges contributed to missing the
20:41
original 2020 elimination target. The
20:45
World Health Organization has now
20:46
extended the global elimination goal to
20:49
2030, recognizing the complexity of
20:52
reaching the final populations. While
20:54
tremendous progress has been made in
20:56
reducing lymphatic feriosis infections
20:58
globally, overcoming the remaining
21:01
challenges will require innovative
21:03
approaches, sustained commitment, and
21:05
targeted strategies for the most
21:07
difficult to reach populations.
21:11
The World Health Organization has
21:13
established ambitious goals for 2030 to
21:16
achieve global elimination of lymphatic
21:18
feriosis as a public health problem.
21:21
after the original 2020 target was not
21:24
met. These revised goals provide a clear
21:26
roadmap for the final push toward
21:28
elimination.
21:30
The World Health Organization has
21:32
outlined three specific measurable goals
21:34
that will determine success in the fight
21:37
against this neglected tropical disease.
21:40
The first goal requires that 80% of all
21:43
countries where lymphatic ferasis is
21:45
endemic must meet the strict validation
21:48
criteria for elimination.
21:50
This means demonstrating that
21:52
transmission has been interrupted and
21:55
the disease is no longer a public health
21:57
problem. Out of every 10 endemic
21:59
countries, at least eight must
22:01
successfully achieve elimination status.
22:04
This represents a significant milestone
22:06
in the global effort. The second goal
22:09
demands that 100% of endemic countries
22:12
establish robust postmass drug
22:14
administration surveillance systems.
22:17
This ensures that even after treatment
22:19
programs end, countries continue
22:21
monitoring to prevent the disease from
22:23
returning. PostMDA surveillance involves
22:26
systematic monitoring through
22:28
transmission assessment surveys and
22:30
ongoing vigilance to detect any signs of
22:32
disease recurrence. This continuous
22:35
watchfulness is essential for
22:37
maintaining elimination status.
22:40
The third and most ambitious goal is to
22:42
reduce to zero the total global
22:44
population requiring mass drug
22:46
administration.
22:48
This means that transmission has been
22:49
interrupted everywhere and no
22:52
communities need preventive treatment.
22:54
Achieving zero population requiring MDA
22:57
represents the ultimate victory over
22:58
lymphatic falariosis. A world where no
23:02
one needs preventive treatment because
23:03
the disease no longer threatens any
23:05
community.
23:08
These three interconnected goals form a
23:10
comprehensive strategy for eliminating
23:12
lymphatic valerasis by 2030. Together,
23:16
they ensure not only that transmission
23:18
is stopped, but that elimination is
23:20
sustained through ongoing surveillance
23:22
and monitoring. The 2030 timeline
23:25
represents humanity's commitment to
23:27
ending the suffering caused by lymphatic
23:29
valeriosis.
23:30
Success will require coordinated global
23:33
effort, sustained funding, and
23:35
unwavering dedication to reaching every
23:37
affected community. Traditional mass
23:40
drug administration programs have made
23:42
significant progress, but some countries
23:45
needed a faster approach to eliminate
23:46
lymphatic feriosis. This led to the
23:49
development of triple drug therapy known
23:51
as IDA.
23:53
IDA stands for three powerful
23:55
antiparasitic drugs used together.
23:57
Ivormectin, dialarbamazine, and
24:00
albendazole. Each drug targets the
24:02
parasite in different ways, making the
24:04
combination much more effective. Let's
24:07
examine the chemical structures of these
24:09
three drugs to understand how they work
24:12
together to eliminate the parasites more
24:14
effectively than traditional two drug
24:17
combinations. Ivormectin is a
24:19
macrocyclic lactone that works by
24:21
binding to glutamate gated chloride
24:23
channels in the parasites nervous system
24:25
causing paralysis of both microfilaria
24:28
and adult worms. DiLarbamazine or DEEC
24:32
is highly effective against microfaria
24:34
and also damages adult worms. It works
24:37
by altering the parasite surface making
24:39
it more susceptible to the host's immune
24:41
system. Albendazole is a benzyazole
24:44
compound that disrupts the parasite
24:46
cellular metabolism by inhibiting
24:49
tubulin polymerization preventing proper
24:51
cell division and function.
24:54
Traditional programs use two drugs at a
24:56
time either DEEC with alendazole or
24:59
ivormectin with albendazole. The triple
25:02
therapy approach combines all three
25:03
drugs creating a synergistic effect that
25:06
clears infections much faster. Studies
25:09
have shown that triple drug therapy can
25:11
clear infections in half the time of
25:13
traditional dual therapy, reducing the
25:16
number of treatment rounds needed and
25:18
accelerating progress toward
25:20
elimination.
25:22
Several countries have begun
25:23
implementing triple drug therapy in
25:25
select districts.
25:27
Papua New Guinea and Fiji were among the
25:29
first to adopt this approach, followed
25:31
by pilot programs in Indonesia and
25:33
India. The benefits are clear. Faster
25:36
elimination means fewer treatment
25:38
rounds, reduced program costs, and
25:41
earlier achievement of elimination
25:42
goals. This accelerated approach is
25:45
helping countries reach the WH target of
25:48
elimination by 2030.
25:51
Triple drug therapy represents a major
25:53
advancement in lymphatic feriosis
25:55
elimination. By combining Ivormectin,
25:58
dialarbamazine and alendazole, countries
26:01
can achieve elimination goals faster and
26:03
more efficiently than ever before.
26:05
Preventing lymphatic feriosis requires a
26:08
comprehensive approach targeting
26:10
multiple aspects of transmission. The
26:12
key is to break the cycle between
26:15
mosquitoes and humans while reducing the
26:17
parasite reservoir in affected
26:19
populations. Prevention strategies focus
26:22
on three main pillars. First,
26:25
controlling mosquitoes to reduce
26:26
transmission. Second, mass drug
26:29
administration to eliminate parasites
26:31
from the population. Third, improving
26:33
sanitation and hygiene to reduce
26:35
favorable conditions for mosquito
26:37
breeding. Bed nets are one of the most
26:40
effective tools for preventing mosquito
26:41
bites. Longlasting insecticidal nets
26:44
provide a physical barrier while also
26:47
killing mosquitoes that come into
26:48
contact with them. They are especially
26:51
important during nighttime hours when
26:53
many feriosis transmitting mosquitoes
26:55
are most active.
26:57
Environmental control involves targeted
26:59
insecticide applications to reduce
27:02
mosquito populations.
27:04
Indoor residual spraying treats walls
27:06
and surfaces where mosquitoes rest.
27:09
Larvides target breeding sites to
27:11
prevent mosquito development. These
27:13
communitywide interventions complement
27:15
personal protection measures. Mass drug
27:18
administration is a cornerstone of
27:20
lymphatic feriosis elimination. Entire
27:23
at risk populations receive annual
27:25
treatment with antifilarial drugs. This
27:28
strategy reduces the number of
27:30
microfilaria circulating in people's
27:32
blood, breaking the transmission cycle
27:34
by preventing mosquitoes from picking up
27:36
the parasites when they bite. Improving
27:39
sanitation and hygiene creates
27:41
unfavorable conditions for mosquito
27:43
breeding. Proper water storage, drainage
27:46
systems, and waste management eliminate
27:49
standing water where mosquitoes lay
27:50
eggs. Personal hygiene practices and
27:53
community cleanliness further reduce
27:55
transmission risks and support overall
27:58
health. Prevention of lymphatic
28:00
valeriosis requires coordinated efforts
28:03
at individual and community levels.
28:05
Personal protection through bed nets and
28:08
repellents, participation in mass drug
28:10
administration programs, elimination of
28:13
mosquito breeding sites, and maintaining
28:16
good hygiene all contribute to breaking
28:18
the transmission cycle and protecting
28:20
communities from this debilitating
28:22
disease. Several key factors determine
28:25
how effectively wukaria bankrofty
28:27
spreads from mosquitoes to humans.
28:30
Understanding these transmission factors
28:32
is essential for developing targeted
28:34
control strategies. The first major
28:37
factor is mosquito density and vector
28:39
distribution. Different mosquito species
28:42
carry the parasite in different regions
28:45
and their population density directly
28:47
affects transmission rates. Human
28:49
behavior plays a crucial role in
28:51
transmission. Activities that increase
28:53
exposure to mosquito bites, such as
28:55
outdoor work during peak biting hours,
28:58
inadequate protective measures, and poor
29:00
housing conditions, all increase
29:02
infection risk. Environmental conditions
29:05
significantly impact transmission.
29:07
Mosquitoes need standing water to breed,
29:10
and factors like temperature, humidity,
29:12
and rainfall patterns all influence
29:14
mosquito survival and reproduction
29:16
rates. Climate change is altering
29:18
transmission patterns worldwide. Rising
29:21
temperatures expand mosquito habitats to
29:24
higher altitudes and latitudes, while
29:26
changing precipitation patterns create
29:28
new breeding opportunities in some areas
29:30
and eliminate them in others.
29:33
Urbanization creates unique transmission
29:35
dynamics. Dense populations provide more
29:38
hosts for the parasite. While urban
29:40
environments often create ideal mosquito
29:43
breeding sites through poor drainage and
29:45
water storage practices.
29:47
Understanding these transmission factors
29:50
helps public health officials design
29:52
targeted interventions.
29:54
Effective control strategies must
29:56
address mosquito breeding sites, promote
29:59
protective behaviors, and adapt to
30:01
changing environmental conditions caused
30:03
by climate change and urbanization.
30:05
Morbidity management and disability
30:07
prevention or MMDP represents a crucial
30:11
pillar in the fight against lymphatic
30:13
feriosis. While treatment can eliminate
30:15
the parasites, many people already
30:17
suffer from chronic complications that
30:19
require ongoing care and management.
30:22
Lymphatic faliasis can cause progressive
30:24
lympadeema where fluid builds up in
30:27
tissues causing swelling. As we can see
30:30
here, the condition progresses from a
30:32
normal foot to mild swelling and
30:34
eventually to severe lympadeema with
30:36
significant disability.
30:39
MMDP focuses on four key components that
30:42
work together to manage symptoms and
30:44
prevent complications. These are
30:46
hygiene, skin care, exercise, and limb
30:49
elevation. Each component plays a vital
30:51
role in maintaining health and
30:53
preventing secondary infections.
30:55
Self-care at home is essential for
30:57
managing lympadeema. Patients can learn
31:00
simple techniques that significantly
31:02
improve their quality of life. Regular
31:04
hygiene, gentle exercises, proper skin
31:07
care, and limb elevation can be done at
31:09
home with proper education and support.
31:13
Specific exercises designed for
31:15
lympadeema patients help improve
31:17
lymphatic drainage and reduce swelling.
31:20
These gentle movements activate the
31:22
muscle pump mechanism, which helps move
31:24
lymphatic fluid and prevents it from
31:26
accumulating in tissues.
31:29
Lympadema causes significant skin
31:31
changes that increase the risk of
31:33
secondary infections. The skin becomes
31:35
thickened, hardened, and more
31:37
susceptible to bacterial and fungal
31:39
infections. Proper skin care with daily
31:42
washing, moisturizing, and wound care is
31:44
essential to prevent these
31:46
complications.
31:48
Access to proper MMDP care is essential
31:51
for improving quality of life. This
31:53
requires training healthare workers,
31:56
establishing community support programs,
31:58
and teaching patients and families how
32:00
to provide care at home. Without access
32:03
to these services, people with
32:04
lympadeema face unnecessary suffering
32:07
and disability.
32:09
MMDP is a vital component of lymphatic
32:11
feriosis control that focuses on
32:13
improving the lives of those already
32:15
affected. Through proper hygiene, skin
32:18
care, exercise, and limb elevation,
32:21
patients can manage their symptoms and
32:22
prevent complications. Most importantly,
32:25
access to education and care ensures
32:28
that no one has to suffer unnecessarily
32:30
from this preventable disability.
32:34
Within every Wrangi worm lives a hidden
32:37
partner, tiny bacteria called Wulbakia.
32:41
These microscopic organisms play a
32:43
crucial role in the worm survival and
32:45
have opened up new possibilities for
32:46
treatment.
32:48
Symbiosis is a close relationship
32:50
between two different organisms. In this
32:53
case, wbakia bacteria live inside the
32:55
worm's body, creating what scientists
32:57
call an endo symbiotic relationship.
33:01
Under a microscope, we can actually see
33:03
these wbakia bacteria living inside the
33:06
worm's tissues. The arrows in this image
33:08
point to the bacteria which appear as
33:11
dark spots within the worm's body.
33:14
Wbakia bacteria are not just passengers.
33:17
They are essential partners. The worms
33:19
depend on these bacteria for
33:20
reproduction, development, and survival.
33:23
Remove the bacteria and the worm dies.
33:27
Scientists discovered they could target
33:29
wbakia bacteria with antibiotics like
33:31
doxycycline. Since the worms depend on
33:34
these bacteria, killing the bacteria
33:36
effectively kills the worms too.
33:39
Understanding the role of wbakia
33:41
bacteria has opened up new treatment
33:44
possibilities. By targeting these
33:46
essential bacterial partners, we can
33:49
fight the infection in a completely
33:51
different way than traditional
33:52
approaches.
33:55
Drug resistance represents one of the
33:57
most serious potential threats to
33:59
eliminating lymphatic feriosis
34:01
worldwide. Understanding and monitoring
34:04
this threat is crucial for maintaining
34:06
our progress against wukaria bankrofti.
34:10
For decades, we have relied on three
34:12
main drugs to fight lymphatic feriosis.
34:15
DEEC, Albendazole, and Ivormectin. These
34:18
medications have been highly effective
34:20
in mass drug administration programs
34:22
worldwide. The World Health Organization
34:24
has established specific treatment
34:26
strategies for different regions as
34:28
shown in this comprehensive table. These
34:31
protocols have guided successful
34:33
elimination programs globally.
34:36
Under normal circumstances, our drugs
34:39
effectively eliminate the parasites.
34:41
Susceptible worms are killed by the
34:43
medication, leading to successful
34:45
treatment and reduce transmission.
34:48
However, if drug resistance develops,
34:51
the scenario changes dramatically.
34:53
Resistant parasites can survive drug
34:55
treatment, continuing to reproduce and
34:58
spread the resistance genes to their
35:00
offspring.
35:01
Scientists monitor the genetic diversity
35:03
of wukaria bankrofti by analyzing DNA
35:07
sequences from parasite samples. Changes
35:09
in these genetic sequences can indicate
35:12
the development of drug resistance
35:14
mutations.
35:15
A global surveillance network monitors
35:17
parasite populations in endemic regions
35:20
worldwide. This network collects samples
35:22
and analyzes genetic data to detect
35:25
early signs of resistance development
35:27
before it becomes widespread.
35:30
Drug resistance could have devastating
35:32
consequences for elimination efforts.
35:35
Years of progress could be reversed if
35:37
resistant strains become widespread,
35:40
potentially setting back global
35:41
elimination goals by decades.
35:45
The key takeaways are clear. Genetic
35:48
monitoring is essential for early
35:49
detection of resistance. Global
35:52
surveillance networks must remain
35:53
vigilant, and preventing resistance is
35:56
far better than trying to manage it
35:58
after it emerges. Continued research and
36:00
monitoring will be crucial for
36:02
maintaining our progress toward
36:04
elimination.
36:08
While current elimination efforts rely
36:10
on mass drug administration, researchers
36:12
are working on an even more powerful
36:14
tool, vaccines. A prophylactic vaccine
36:17
against lymphatic feriosis could provide
36:20
long-term protection and dramatically
36:22
accelerate global elimination efforts.
36:25
Currently, lymphatic feriosis
36:27
elimination relies on mass drug
36:29
administration programs. While
36:31
effective, this approach requires annual
36:33
treatments, complex logistics, and
36:35
treats infections after they occur. A
36:38
vaccine would represent a paradigm
36:40
shift. A prophylactic vaccine would
36:42
prevent infections before they start,
36:44
potentially providing years of
36:46
protection with just one or a few doses.
36:49
This could dramatically simplify
36:51
elimination programs and provide more
36:53
sustainable protection. Researchers are
36:56
exploring multiple vaccine development
36:58
approaches. This includes recombinant
37:00
vector vaccines, DNA vaccines, and small
37:03
molecule approaches. Each method has
37:05
different advantages in terms of safety,
37:07
efficacy, and manufacturing. Several
37:10
vaccine candidates are currently in
37:12
development. Antigen-based vaccines
37:14
target specific parasite proteins that
37:17
could trigger protective immunity. DNA
37:19
vaccines deliver genetic material that
37:22
instructs cells to produce these
37:23
antigens. Vector vaccines use modified
37:27
viruses to deliver the vaccine
37:28
components. A lymphatic feriosis vaccine
37:31
would work by training the immune system
37:34
to recognize and fight the parasite.
37:36
When vaccinated, the immune system
37:38
produces antibodies and memory cells
37:41
that provide longlasting protection.
37:43
When a mosquito carrying the parasite
37:45
bites a vaccinated person, the
37:47
pre-existing antibodies and activated
37:50
immune cells quickly recognize and
37:52
eliminate the parasite before it can
37:54
establish infection. This prevents the
37:56
disease from developing entirely.
37:59
Developing a vaccine for lymphatic
38:00
feriosis faces several significant
38:03
challenges. The parasite has a complex
38:06
life cycle with multiple stages making
38:08
it difficult to identify the best
38:10
targets for immune protection. Safety
38:12
testing must be thorough across diverse
38:14
populations and the development timeline
38:17
is lengthy. Clinical trials alone could
38:20
take 5 to 8 years with a realistic goal
38:23
of having vaccines available by the late
38:25
2030s. Vaccine development represents
38:28
the future of lymphatic feriosis
38:30
prevention. While challenges exist,
38:33
successful vaccines could provide long-
38:35
lasting protection, simplify elimination
38:37
programs, and accelerate the goal of
38:39
global elimination. Research continues
38:42
with promising candidates in the
38:43
pipeline.
38:45
Real world case studies show us both the
38:47
remarkable successes and ongoing
38:49
challenges in eliminating lymphatic
38:51
feriosis.
38:53
These examples teach us valuable lessons
38:55
about what works and what obstacles
38:57
remain. Let's start with the success
38:59
stories. Several countries have achieved
39:01
remarkable progress in eliminating
39:04
lymphatic feriosis as a public health
39:06
problem. This world map shows the global
39:09
status of lymphatic feriosis elimination
39:11
efforts. The different colors represent
39:14
various stages of progress from
39:16
countries still implementing mass drug
39:18
administration to those that have
39:20
successfully eliminated the disease.
39:24
Costa Rica, Suriname, and Trinidad and
39:26
Tobago were among the first countries to
39:29
achieve elimination. In 2011, these
39:32
three nations were officially removed
39:34
from the World Health Organization's
39:36
list of endemic countries.
39:39
India has set an ambitious goal to
39:41
eliminate lymphatic feriosis by 2027, 3
39:45
years ahead of the global target. The
39:47
country has launched comprehensive
39:49
strategies including mission mode mass
39:51
drug administration, morbidity
39:53
management and innovative approaches.
39:57
However, the fight against lymphatic
39:59
valeriosis is not without challenges.
40:02
Some countries face setbacks that remind
40:04
us why continued vigilance is essential.
40:07
Colombia provides a cautionary tale.
40:09
Despite previous progress, a recent case
40:11
of lymphatic ferasis was detected in the
40:14
country. This highlights how
40:16
urbanization, migration, and reduced
40:18
surveillance can potentially lead to
40:20
reemergence of the disease.
40:23
These case studies teach us important
40:25
lessons. Successful programs require
40:28
sustained mass drug administration, high
40:31
population coverage, strong health care
40:33
infrastructure, and political
40:35
commitment. However, even after
40:37
elimination, ongoing risks like
40:39
population movement and reduced
40:40
surveillance can threaten progress. True
40:43
success requires both elimination and
40:46
sustained vigilance. The global health
40:48
community has reached clear consensus on
40:50
the massive impact of lymphatic
40:52
feriosis.
40:53
Let's examine the key statistics and
40:56
expert opinions that shape our
40:58
understanding of this disease. According
41:00
to the World Health Organization and
41:02
leading parasettologists, lymphatic
41:04
ferasis stands as one of the world's
41:07
leading causes of permanent disability.
41:09
This places it among the most
41:11
significant neglected tropical diseases
41:13
affecting human health. The numbers are
41:16
staggering. Current estimates show that
41:19
approximately 120 million people
41:21
worldwide are actively infected with
41:24
lymphatic feriosis while nearly 900
41:27
million people remain at risk of
41:29
infection. Among the three species that
41:31
cause lymphatic feriosis, wukaria
41:34
bankrofti is overwhelmingly dominant.
41:37
Expert analysis shows that this single
41:39
species accounts for approximately 90%
41:41
of all lymphatic feriosis cases
41:44
globally. This global distribution map
41:46
from the World Health Organization shows
41:49
the endemic countries and the status of
41:51
preventive chemotherapy programs. The
41:54
varying colors indicate different stages
41:56
of elimination efforts across affected
41:58
regions. The economic analysis by health
42:01
economists reveals remarkable benefits
42:03
from elimination efforts. The global
42:06
program to eliminate lymphatic feriosis
42:09
generated an estimated $ 24 billion in
42:12
economic benefits between 2000 and 2007
42:15
alone. Beyond statistics, experts
42:18
emphasize the human cost. This clinical
42:21
image shows the severe lympadema that
42:23
affects millions. The baseline estimates
42:26
indicate 25 million men suffer from
42:28
hydroil while over 15 million people
42:30
live with lympadeema. The global health
42:33
community agrees lymphatic feriosis
42:35
represents one of the most significant
42:37
yet preventable causes of disability
42:40
worldwide. With coordinated efforts,
42:42
these devastating statistics can become
42:45
history, transforming millions of lives
42:47
in the process. We've covered a lot of
42:50
ground in our exploration of wukaria
42:52
bangfi and lymphatic feriosis. Let's
42:56
summarize the most important points and
42:58
key takeaways from our journey. First,
43:00
weria bankrofti represents a major
43:03
global health challenge. This parasitic
43:05
worm infects 120 million people
43:07
worldwide with 856 million more at risk.
43:11
It's a leading cause of disability
43:13
causing severe conditions like
43:15
elephantiasis where limbs become
43:17
massively swollen and hydrail affecting
43:19
men's reproductive health. Second, the
43:22
parasite has a complex life cycle
43:24
involving both mosquitoes and humans.
43:28
Mosquitoes serve as essential vectors
43:30
picking up microfilaria from infected
43:32
blood and transmitting infective larae
43:34
to new hosts. Adult worms then mature in
43:37
the human lymphatic system where they
43:39
can live for years continuously
43:41
producing microfilaria that circulate in
43:43
the bloodstream.
43:45
Third, we have effective tools to fight
43:47
this disease. Treatment options include
43:50
DEEC, alendazol and Ivormectin with
43:52
newer triple drug therapy showing
43:54
promise for faster elimination.
43:56
Prevention strategies focus on mass drug
43:58
administration to entire at risk
44:00
populations, mosquito control measures,
44:02
bed nets, and community education about
44:05
the disease.
44:07
Fourth, the global elimination program
44:09
is making remarkable progress. Since
44:12
2000, 9.7 billion treatments have been
44:15
delivered worldwide, leading to a 74%
44:18
reduction in infections.
44:20
The World Health Organization has set an
44:22
ambitious but achievable target of
44:24
eliminating lymphatic ferasis as a
44:26
public health problem by 2030. In
44:29
conclusion, while Wukareia bankrupty has
44:32
caused immense suffering throughout
44:34
human history, we now have the knowledge
44:36
and tools to defeat it. With continued
44:39
global cooperation, effective
44:41
treatments, and comprehensive prevention
44:43
strategies, we can eliminate lymphatic
44:46
feriosis and free millions of people
44:48
from this ancient disease.
44:51
Thank you for joining us on this
44:52
educational journey about one of
44:54
humanity's most persistent parasitic
44:56
enemies.